Filter
12506
Filtered Results: 12506
Text search:
audit
Featured
Recommendations
1025
New Publications
3258
Language
Document type
No document type
7117
Studies & Reports
2112
Guidelines
1445
Manuals
600
Strategic & Response Plan
397
Fact sheets
322
Training Material
225
Situation Updates
154
Resource Platforms
51
Infographics
37
Brochures
26
Online Courses
13
Videos
6
App
1
Countries / Regions
India
558
Global
466
Kenya
337
Ethiopia
261
South Africa
250
Sierra Leone
249
Liberia
227
Nigeria
227
Nepal
227
Uganda
223
Myanmar / Burma
213
Western and Central Europe
207
Rwanda
175
Malawi
173
Bangladesh
169
Latin America and the Carribbean
169
Syria
168
Africa
168
Zambia
162
Tanzania
156
Congo, Democratic Republic of
145
Ghana
143
Ukraine
143
Philippines
108
Senegal
100
South Sudan
91
Mozambique
86
Namibia
85
Zimbabwe
84
Guinea
82
Cambodia
78
West and Central Africa
78
Indonesia
76
Haiti
73
East and Southern Africa
73
Brazil
71
Lesotho
71
Burkina Faso
69
Eastern Europe
69
South–East Asia Region
68
Germany
67
Venezuela
67
Yemen
62
Asia
60
Benin
59
Middle East and North Africa
55
Colombia
53
Cameroon
48
Botswana
47
Pakistan
43
Afghanistan
42
Russia
41
Paraguay
40
Eastern Europe and Central Asia
39
Mali
38
Central African Republic
36
Lebanon
32
Eswatini/ Swaziland
32
Somalia
28
Jordan
28
Sudan
25
Argentina
25
Côte d’Ivoire / Ivory Coast
24
Thailand
23
Madagascar
23
Vietnam
23
Iraq
21
Western Pacific Region
21
USA
20
Peru
20
Chile
18
Niger
17
Turkey
17
Bolivia
17
Tajikistan
17
China
16
Angola
15
Moldova
15
Laos
14
Burundi
13
Ecuador
13
Palestine
13
Albania
13
Sri Lanka
12
Georgia
12
Iran
11
North Macedonia
10
Libya
10
Southern Africa
10
Chad
9
Greece
9
North America
9
Togo
8
Papua New Guinea
8
Kyrgyzstan
8
Egypt
7
Malaysia
7
Mexico
7
Armenia
7
United Kingdom
7
Spain
7
Guinea-Bissau
6
Serbia
6
Honduras
6
El Salvador
6
Bhutan
6
Kazakhstan
6
Portugal
6
Morocco
5
Hungary
5
Poland
5
Italy
5
Canada
5
Timor Leste/ East Timor
5
Uzbekistan
5
Turkmenistan
5
Jamaica
5
Saudi Arabia
4
Gambia
4
Guatemala
4
Fiji
4
Djibouti
4
Japan
4
Tunisia
4
Belarus
4
Ireland
3
Vanuatu
3
Dominican Republic
3
Croatia
3
Estonia
3
Romania
3
Belgium
3
Bosnia and Herzegovina
3
Singapore
2
Nicaragua
2
Other region
2
North Korea
2
Congo-Brazzaville
2
Qatar
2
Bulgaria
2
Lithuania
2
Australia
2
Gabon
2
Denmark
2
France
2
Mauritius
2
Azerbaijan
2
Israel
2
Mauritania
1
Switzerland
1
Cape Verde
1
Luxembourg
1
Solomon Islands
1
Slovakia
1
Uruguay
1
Maldives
1
Norway
1
South Korea
1
Algeria
1
Morocco
1
Latvia
1
Authors & Publishers
Publication Years
Category
Countries
4691
Clinical Guidelines
862
Women & Child Health
633
Public Health
614
Key Resources
561
Capacity Building
260
Pharmacy & Technologies
126
Annual Report MEDBOX
3
Toolboxes
COVID-19
1160
Mental Health
944
HIV
876
TB
566
Disability
550
Planetary Health
457
Ebola
404
Conflict
404
Rapid Response
344
Caregiver
344
AMR
331
Refugee
274
NTDs
261
NCDs
232
Pharmacy
205
Natural Hazards
189
Global Health Education
185
Health Financing Toolbox
136
Zika
106
Specific Hazards
83
Cholera
82
Polio
71
Social Ethics
56
Typhoon
11
South Sudan
3
Health Financing
3

In 2024, we need US$1.5 billion to provide live-saving health care to millions of people in emergencies. An alarming combination of conflict, climate-related threats and increasing economic hardship mean an estimated 166 million people require health assistance.

The 2019-2023 Strategy for UNU-IIGH, developed in
2018, built on UNU-IIGH’s strategic advantage and
position vis-à-vis the UN and global health ecosystem.
The Strategy set a goal to advance evidencebased policy on key issues related to sustainable
development and health and shifted the Instit...

Global cardiovascular disease (CVD) burden is high and rising, especially in low-income and middle-income countries (LMICs). Focussing on 45 LMICs, we aimed to determine (1) the adult population’s median 10-year predicted CVD risk, including its variation within countries by socio-demographic char...
A major problem facing the world is how to build peace following the ravages of increasingly protracted armed conflict. Armed conflicts leave behind shattered, divided societies that are at risk of repeating cycles of violence, and therefore need concerted peacebuilding efforts. Conflicts also take ...

This document contains guidance for strengthening the disability inclusiveness of MHPSS responses and programmes in emergency settings. It is intended to supplement the IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings (2007).
Overall Objective
To consider and add...

Introduction Community health workers (CHWs) are increasingly being tasked to prevent and manage cardiovascular disease (CVD) and its risk factors in underserved populations in low-income and middle-income countries (LMICs); however, little is known about the required training necessary for them to ...

The cardiovascular disease continuum begins with risk factors such as diabetes mellitus (DM), progresses to vasculopathy and myocardial dysfunction, and finally ends with cardiovascular death. Diabetes is associated with a 2- to 4-fold increased risk for heart failure (HF). Moreover, HF patients wit...
Laboratory manual for yellow fever
recommended
This WHO laboratory manual provides the most up to date methods and procedures for the laboratory identification of yellow fever virus infection in humans. It provides guidance on the establishment and maintenance of an effective laboratory providing routine surveillance testing for yellow fever, wh...

In this version of the compendium, each guidance is coded using the International Classification of Health Interventions (ICHI).
The compendium provides a systematic compilation of published guidance from WHO and other UN organizations on health and environment. Guidance on policies and actions a...
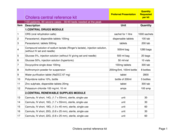
Humanitarian crises exacerbate nutritional risks and often lead to an increase in acute malnutrition. Emergencies include both manmade (conflict) and natural disasters (floods, drought, cyclones, typhoons, earthquakes, volcanic eruptions, etc.). Complex emergencies are combinations of both manmade a...
Myocardial infarctions are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI), based on changes in ECG. When blood flow to a part of the heart stops or the heart is injured and fails to receive enough oxygen required for its adequate functioning the conditi...

WHO has published the first-ever guidance on the clinical management of diphtheria. The only previously available guidance was an operational protocol. The new guidance followed the rigorous process for developing guidance at WHO.
It addresses the use of Diphtheria Antitoxin (DAT) in the treatmen...

The ERF provides WHO staff with essential guidance on how the Organization manages the assessment, grading and response to public health events and emergencies with health consequences, in support of Member States and affected communities. The ERF adopts an all-hazards approach and it is therefore a...

A sanitary inspection is a simple, on-site evaluation (traditionally using a checklist) to help identify and support the management of priority risk factors that may lead to contamination of a drinking-water supply. Sanitary inspections are a well-established and widely-applied practice. They can su...

Diphtheria is caused by Corynebacterium species, mostly by toxin-producing Corynebacterium diphtheriae and rarely by toxin-producing strains of C. ulcerans and C. pseudotuberculosis. The most common type of diphtheria is classic respiratory diphtheria, whereby the exotoxin produced characteristicall...
The Global Burden of Disease Study (GBD) began 30 years ago with the goal of providing timely, valid and relevant assessments of critical health outcomes. Over this period, the GBD has become progressively more granular. The latest iteration provides assessments of thousands of outcomes for diseases...
Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among...

Non-communicable diseases (NCDs) are of increasing concern for society and national governments, as well as globally due to their high mortality rate. The main risk factors of NCDs can be classified into the categories of self-management, genetic factors, environmental factors, factors of medical co...

As the Americas undergo profound demographic change and there are more persons aged 65 years or older than children younger than 5 years, it is crucial to recognize that national immunization programs must be redesigned to ensure comprehensive protection for individuals across the lifespan. By adopt...