Filter
11263
Filtered Results: 11263
Text search:
stratégie
Featured
Recommendations
892
New Publications
2971
Language
Document type
No document type
6245
Studies & Reports
1936
Guidelines
1315
Strategic & Response Plan
536
Manuals
532
Fact sheets
275
Training Material
169
Situation Updates
106
Resource Platforms
50
Infographics
37
Brochures
28
Online Courses
26
Videos
4
Dashboards/Maps
2
App
2
Countries / Regions
Global
453
India
409
Kenya
319
Ethiopia
232
Uganda
208
South Africa
207
Nepal
201
Nigeria
196
Indonesia
194
Western and Central Europe
191
Sierra Leone
189
Liberia
183
Myanmar / Burma
183
Latin America and the Carribbean
174
Africa
165
Malawi
154
Rwanda
152
Congo, Democratic Republic of
151
Zambia
148
Tanzania
147
Bangladesh
142
Syria
138
Germany
132
Ghana
124
Ukraine
111
Senegal
110
Brazil
93
South Sudan
82
Venezuela
82
Philippines
80
Mozambique
79
Burkina Faso
77
Namibia
77
Eastern Europe
76
Russia
76
Guinea
73
Haiti
72
West and Central Africa
72
Lesotho
67
East and Southern Africa
67
Cambodia
65
Zimbabwe
64
Middle East and North Africa
64
Asia
62
Benin
60
South–East Asia Region
60
Colombia
58
Yemen
53
Paraguay
52
Cameroon
51
Argentina
47
Peru
46
Botswana
46
Central African Republic
43
Lebanon
35
Pakistan
33
Afghanistan
33
Eastern Europe and Central Asia
33
Sudan
28
Mali
26
Eswatini/ Swaziland
26
Bolivia
26
Madagascar
26
Chile
26
Thailand
23
Somalia
21
Jordan
21
Western Pacific Region
21
Tajikistan
20
USA
19
Ecuador
19
Côte d’Ivoire / Ivory Coast
17
El Salvador
17
Vietnam
17
Angola
16
Niger
15
Iraq
15
China
15
Sri Lanka
13
Albania
13
Laos
13
Moldova
13
Guinea-Bissau
12
Burundi
11
North America
11
Turkey
10
Papua New Guinea
10
Georgia
10
Chad
9
Palestine
9
Italy
9
Southern Africa
9
Togo
8
North Macedonia
7
Libya
7
Kyrgyzstan
7
Hungary
6
Honduras
6
Timor Leste/ East Timor
6
Iran
6
Kazakhstan
6
Jamaica
6
Portugal
6
Morocco
5
Saudi Arabia
5
Egypt
5
Gambia
5
Mexico
5
Bhutan
5
Poland
5
Armenia
5
Romania
5
Uzbekistan
5
Turkmenistan
5
Tunisia
5
United Kingdom
5
Spain
5
Malaysia
4
Switzerland
4
Guatemala
4
Estonia
4
Japan
4
Belarus
4
Singapore
3
Serbia
3
Canada
3
Uruguay
3
France
3
Mauritius
3
Bosnia and Herzegovina
3
Ireland
2
Dominican Republic
2
Croatia
2
Greece
2
Nicaragua
2
Other region
2
Fiji
2
Djibouti
2
Mongolia
2
Qatar
2
Bulgaria
2
Lithuania
2
Slovakia
2
Gabon
2
Belgium
2
Israel
2
Austria
1
North Korea
1
Denmark
1
Maldives
1
Norway
1
Algeria
1
Morocco
1
Azerbaijan
1
French Guyana
1
Eritrea
1
Authors & Publishers
Publication Years
Category
Countries
4688
Clinical Guidelines
657
Public Health
594
Women & Child Health
493
Key Resources
461
Capacity Building
207
Pharmacy & Technologies
63
Annual Report MEDBOX
3
Toolboxes
COVID-19
1070
HIV
817
Mental Health
813
TB
614
Planetary Health
455
Disability
440
Conflict
312
AMR
305
Ebola
289
Rapid Response
287
Caregiver
261
NCDs
243
NTDs
238
Refugee
234
Global Health Education
221
Natural Hazards
136
Pharmacy
123
Health Financing Toolbox
100
Zika
73
Polio
68
Cholera
67
Specific Hazards
50
Social Ethics
47
Typhoon
7
Health Financing
3
South Sudan
2
Background
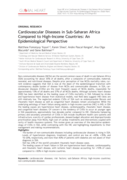
Cardiovascular diseases (CVDs) are one of the global leading causes of concern due to the rising prevalence and consequence of mortality and disability with a heavy economic burden. The objective of the current study was to analyze the trend in CVD incidence, mortality, and mortality-to-...
In 2015, the United Nations set important targets to reduce premature
cardiovascular disease (CVD) deaths by 33% by 2030. Africa disproportionately
bears the brunt of CVD burden and has one of the highest risks of dying
from non-communicable diseases (NCDs) worldwide. There is currently
an epide...

Global cardiovascular disease (CVD) burden is high and rising, especially in low-income and middle-income countries (LMICs). Focussing on 45 LMICs, we aimed to determine (1) the adult population’s median 10-year predicted CVD risk, including its variation within countries by socio-demographic char...
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...

This document contains guidance for strengthening the disability inclusiveness of MHPSS responses and programmes in emergency settings. It is intended to supplement the IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings (2007).
Overall Objective
To consider and add...
Laboratory manual for yellow fever
recommended
This WHO laboratory manual provides the most up to date methods and procedures for the laboratory identification of yellow fever virus infection in humans. It provides guidance on the establishment and maintenance of an effective laboratory providing routine surveillance testing for yellow fever, wh...

In this version of the compendium, each guidance is coded using the International Classification of Health Interventions (ICHI).
The compendium provides a systematic compilation of published guidance from WHO and other UN organizations on health and environment. Guidance on policies and actions a...

WHO has published the first-ever guidance on the clinical management of diphtheria. The only previously available guidance was an operational protocol. The new guidance followed the rigorous process for developing guidance at WHO.
It addresses the use of Diphtheria Antitoxin (DAT) in the treatmen...

The ERF provides WHO staff with essential guidance on how the Organization manages the assessment, grading and response to public health events and emergencies with health consequences, in support of Member States and affected communities. The ERF adopts an all-hazards approach and it is therefore a...

Background
Noncommunicable diseases are major contributors to morbidity and mortality worldwide. Modifying the risk factors for these conditions, such as physical inactivity, is thus essential. Addressing the context or circumstances in which physical activity occurs may promote physical activity a...

Diphtheria is caused by Corynebacterium species, mostly by toxin-producing Corynebacterium diphtheriae and rarely by toxin-producing strains of C. ulcerans and C. pseudotuberculosis. The most common type of diphtheria is classic respiratory diphtheria, whereby the exotoxin produced characteristicall...

The Guidelines for drinking-water quality: small water supplies have been developed to address the needs and opportunities associated with small supplies to facilitate progressive improvement towards safe and sustainable drinking-water services for all. These Guidelines are based on the principal re...

Mental health problems are common and cause great suffering to individuals and communities around the world. They have a significant impact not only on the physical and mental health of those affected but also on their families and the communities they live in. At the same time, all communities have...
Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among...

Objective: To identify gaps in national stroke guidelines that could be bridged to enhance the quality of stroke care services in low- and
middle-income countries.
Methods: We systematically searched medical databases and websites of medical societies and contacted international organizations.
Co...
Around the world, more than 2 billion people lack access to safely managed water, sanitation and hygiene services, with conflicts and climate change exacerbating the issue.
Unsafe and insufficient WASH facilities, especially in rural and remote areas, can lead to increased health complications fo...
Through technical consultations with countries and partners, WHO has led the development of Preparedness and Resilience for Emerging Threats Module 1: Planning for respiratory pathogen pandemics. Version 1.0. The Module, currently available as an advanced draft, builds on previous pandemic lessons a...
The World Food Programme (WFP) has taken important steps to progress disability inclusion across its programming and operations. In late 2022, WFP commissioned the Nossal Institute, University of Melbourne in partnership with the Faculty of Psychology, Universitas Gadjah Mada, Indonesia to identify ...
Evidence-based psychological interventions are an important part of health, social, protection and education services and can help increase access to effective mental health treatments and progression towards universal health coverage.
This manual provides managers and others responsible for plan...
While epidemiological data for type 1 diabetes (T1D) in low/middle-income countries, and particularly low-income countries (LICs) including Liberia is lacking, prevalence in LICs is thought to be increasing. T1D care in LICs is often impacted by challenges in diagnosis and management. These challeng...