Filter
8766
Text search:
increase
access
Featured
694
2389
Language
8597
175
141
94
90
60
42
28
12
12
11
11
10
9
9
8
8
8
7
7
6
6
6
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
Document type
5000
1688
898
408
326
164
120
96
26
18
15
3
2
1
Countries
373
352
275
208
179
177
172
172
168
161
161
150
139
138
131
131
128
127
124
122
105
97
82
81
71
70
69
68
60
56
55
54
53
52
50
49
47
47
46
42
42
39
38
37
36
34
33
27
27
26
26
26
25
25
24
24
22
20
20
19
18
17
17
16
15
14
14
13
13
13
13
12
12
12
9
9
9
9
9
9
8
8
8
8
7
7
7
6
6
6
6
5
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
985
431
397
247
209
208
179
148
145
81
61
49
46
46
44
42
41
38
38
37
36
34
34
34
34
32
32
32
32
31
31
30
30
30
29
29
28
28
28
28
28
27
25
24
24
23
23
23
22
22
22
20
20
20
20
20
20
19
18
18
17
17
17
17
17
16
16
16
16
16
16
15
15
15
15
14
14
14
14
14
14
13
13
13
13
13
13
12
12
12
12
12
12
12
12
12
12
11
11
11
11
11
11
11
11
11
11
11
10
10
10
10
10
10
10
10
10
10
10
10
9
9
9
9
9
9
9
9
9
9
9
9
9
9
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
7
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Publication Years
1
2405
5570
756
30
3
1
Category
3344
563
491
447
336
162
61
9
4
3
Toolboxes
723
722
643
390
384
363
319
232
211
201
193
189
170
166
163
144
125
108
64
50
45
41
24
8
2
1

The Transformation Agenda (TA) ushered in an ambitious reform process intended to transform the World Health Organization (WHO) into an organization that is proactive, results-driven, accountable and which meets stakeholder expectations, towards transforming and improving public health services in t
...
he African Region. It aimed to achieve a WHO that is pro-results, which optimally and creatively targets technical work as well as make operations more responsive, with greater effectiveness in both communications and partnerships. The Africa Region has been the epicentre of the human immunodeficiency virus (HIV) epidemic and it’s one of the leading causes of disease and death on the continent. The WHO, with partners, has worked tirelessly for many years to control the threat and reduce the negative impact of the disease. Since the early 2000s, significant progress has been made in the global fight against the scourge of HIV. However, the WCA subregion was falling concerningly behind ESA on several key indicators of progress. In 2016, the WHO joined UNAIDS, UNICEF and other partners in a call for a strong and urgent response to support WCA countries to develop catch-up plans to triple and fast-track ART coverage, to enable the region to catch up with ESA by the end of 2020. Implementation of a widespread test-and-treat strategy, coupled with the scale-up of differentiated service delivery (DSD) and mobilization of requisite funding, accelerated WCA’s progress towards this goal. The HIV treatment catch-up and fast-track plan has achieved its target of seeing the West and Central African region (WCA) catch up with the Eastern and Southern African region’s (ESA) antiretroviral coverage rate of 78% in 2021, albeit later than the 2020 target time frame. A 33% improvement was achieved in WCA, against 21% in ESA, between 2015–2020. WCA achieved a significant 42% increase, compared to ESA’s 23%, between 2015 and 2021, to see WCA draw level with ESA at 78%. In the Democratic Republic of the Congo (DRC) alone, progress of up to 47% was observed between 2015 and 2020, for example. In addition, 1.6 million more People Living with HIV (PLHIV) were enrolled on antiretroviral treatment (ART) between 2015 and 2020.
more
Ethiopia has been repeatedly affected by conflict, flooding, drought, and disease outbreaks in the past years. As of January 2024, the country is actively responding to the longest recorded cholera outbreak which started in August 2022, recurrent measles outbreaks which started in August 2021, and t
...
he highest number of malaria cases reported since 2017. The El Niño phenomenon is expected to cause further havoc up to July 2024, by causing drought in some parts of the country, and flooding in others. Food insecurity due to lost harvest and livestock is aggravating already high malnutrition rates, negatively impacting morbidity and mortality.
The Health Cluster is closely collaborating with the Ministry of Health (MOH) to prepare for, prevent, and respond to public health emergencies by mobilizing resources to enable health partners to provide life-saving health services to vulnerable populations.
In an environment with ever-increasing needs and decreased funding, the below priorities for 2024 and 2025 have been identified: 1 Strengthen advocacy for longer-term, development funding to address root causes of recurrent disease outbreaks, including through the Humanitarian-Development-Peace Nexus 2 Advocate for increased access to quality health services, with a strong focus on:
sexual and reproductive health services (including for survivors of sexual and gender-based violence)
inclusion of people with disabilities, older people, and people living with HIV
remote populations through inclusion of Mobile Health Teams (MHT) as part of the health system 3 Standardize health services provided by Health Cluster partners through the implementation of Essential Health Care packages, aligned with existing MOH guidance, aimed at ensuring quality service delivery for affected populations, especially at community level 4 Strengthen quality of, and access to data for needs analysis and informed decision-making 5 Strengthen subnational coordination, with increased focus on zones and local health partners
more

Impact of health systems strengthening on coverage of maternal health services in Rwanda, 2000–2010: a systematic review
Maurice Bucagu, Jean M. Kagubare, Paulin Basinga, Fidèle Ngabo, Barbara K Timmons & Angela C Lee
Reproductive Health Matters
(2012)
CC
From 2000 to 2010, Rwanda implemented comprehensive health sector reforms to strengthen the public health system, with the aim of reducing maternal and newborn deaths in line with Millennium Development Goal 5, among many other improvements in national health. Based on a systematic review of the lit
...
erature, national policy documents and three Demographic & Health Surveys (2000, 2005 and 2010), this paper describes the reforms and the policies they were based on, and provides data on the extent of Rwanda’s progress in expanding the coverage of four key women’s health services. Progress took place in 2000–2005 and became more rapid after 2006, mostly in rural areas, when the national facility-based childbirth policy, performance-based financing, and community-based health insurance were scaled up. Between 2006 and 2010, the following increases in coverage took place as compared to 2000–2005, particularly in rural areas, where most poor women live: births with skilled attendance (77% increase vs. 26%), institutional delivery (146% increase vs. 8%), and contraceptive prevalence (351% increase vs. 150%). The primary factors in these improvements were increases in the health workforce and their skills, performance-based financing, community-based health insurance, and better leadership and governance. Further research is needed to determine the impact of these changes on health outcomes in women and children.
more

Global Tuberculosis Report 2022 Factsheet
recommended
The World Health Organization Global TB Report provides a comprehensive and up-to-date assessment of the TB epidemic, and progress in the response, at global, regional and country levels.
The 2022 edition features data on disease trends and the response to the epidemic from 215 countries and area
...
s, including all 194 World Health Organization (WHO) Member States. It provides a comprehensive and up-to-date assessment of the TB epidemic, progress in the response at global, regional and country levels, as well as on the impact of the COVID-19 pandemic on TB services.
TB remains one of the top infectious killers in the world. This year’s report presents data on an increase in the number of people falling ill with TB and drug resistant TB for the first time in many years. Increases were also reported on the number of TB deaths, highlighting the severe impact of the COVID-19 pandemic and other crises on the TB response that has reversed years of progress. It also presents the status of progress towards targets set at the first-ever United Nations General Assembly high-level meeting on TB in 2018 as well as the targets of the WHO End TB Strategy and the Sustainable Development Goals.
more
While the full extent of Cyclone Ida’s impact is still being assessed, early reports indicate significant damage to infrastructure and livelihoods, with an estimated 3,000km2 of land submerged. Preliminary government reports as of 24 March indicate that more than 58,600 houses have been damaged, i
...
ncluding 36,747 totally destroyed, 19,733 partially destroyed and 2,184 flooded. More than 500,000 hectares of crops have been damaged, which is expected to significantly increase food insecurity given that the flooding has coincided with the annual harvest season. More than 3,100 schools have been damaged, along with at least 45 health centres.
Nearly 110,000 people remained displaced in more than 130 accommodation centres – mostly schools and other public buildings – in Sofala (90), Manica (26), Zambezia (10) and Tete (4), where humanitarian needs are acute and both the risk of communicable disease outbreaks and protection risks – particularly for women and girls – are high
more
The Joint Monitoring Programme (JMP) report – Progress on household drinking water, sanitation and hygiene 2000 - 2020 – presents estimates on household access to safely managed drinking water, sanitation and hygiene services over the past five
...
years, and assesses progress toward achieving the sixth sustainable development goal (SDG) to ‘Ensure availability and sustainable management of water and sanitation for all by 2030’.
more

PLoS ONE 7(12): e52986. doi:10.1371/journal.pone.0052986. Opern Access please download from the website

The New England Journal of Medicine has a perspective on Ebola Virus Disease in West Africa — Clinical Manifestations and Management, written by authors who have cared for more than 700 patients with EVD between August 23 and October 4, 2014, in the largest Ebola treatment unit in Monrovia, Liberi
...
a (Free Access) NEJm, November 5, 2014DOI: 10.1056/NEJMp1413084
more

Guidance on temporary malaria control measures in Ebola-affected countries
World Health Organization
(2014)
Malaria is a prevalent cause of febrile illnesses in areas with high transmission, and its clinical presentation overlaps with initial signs of Ebola disease. For this reason, the effectiveness of the Ebola response in Guinea, Liberia and Sierra Leone can be optimized through the deployment of targe
...
ted measures to reduce the number of fever cases due to malaria
WHO recommends specific adaptations in the diagnosis of malaria and in LLIN distribution in countries heavily affected by the Ebola outbreak and mass drug administration using artemisinin-based combination therapies (ACTs) in areas where transmission of both Ebola and malaria is high and access to malaria treatment is very low.
more

Barriers to HIV Services and Treatment for Persons with Disabilities in Zambia
The 80-page report documents the obstacles faced by people with disabilities in both the community and healthcare settings. These include pervasive stigma and discrimination, lack of
...
access to inclusive HIV prevention education, obstacles to accessing voluntary testing and HIV treatment, and lack of appropriate support for adherence to antiretroviral treatment. The report also describes the sexual and intimate partner violence women and girls with disabilities face, and the need for the government and international donors to do more to ensure inclusive and accessible HIV services.
more
A survey was conducted in countries in all six WHO regions and focused on the building blocks that are considered prerequisites to combat antimicrobial resistance: a comprehensive national plan, laboratory capacity to undertake surveillance for resistant microorganisms,
...
access to safe, effective antimicrobial medicines, control of the misuse of these medicines, awareness and understanding among the general public and effective infection prevention and control programmes.
more

The purpose of this Strategy is to set out the way to meet the needs of the rural populations for improved domestic water supply services, access to and use of improved sanitation with elimination of open defecation, and improved hygiene behaviour b
...
y the Year 2030. It also addresses water, sanitation and hygiene in schools up to high school level and health facilities up to township hospital level. The Strategy is supported by Investment Plans covering a financing period 2015 to 2030 in order to ensure sufficient funding for development and operation of services in accordance with the Strategy.
more
more
Diarrhea is one of the world’s leading causes of child illness and death, and rotavirus is the most common cause of severe diarrhea. Yet it can be prevented and treated. There is a vaccine. And while hundreds of thousands of children in India will gain a
...
ccess to rotavirus vaccines -part of a national introduction marking Asia’s largest so far -millions of children globally still lack access. This new report from the Rota Council summarizes the latest evidence on rotavirus disease and vaccines and identifies 21 recommendations for stakeholders to scale up coverage and prevent hundreds of thousands of child deaths annually.
more
TNew data from the World Health Organization reveal that the COVID-19 pandemic has disrupted malaria services, leading to a marked increase in cases and deaths.
According to WHO’s latest World malaria report, there were an estimated 241 million m
...
alaria cases and 627 000 malaria deaths worldwide in 2020. This represents about 14 million more cases in 2020 compared to 2019, and 69 000 more deaths. Approximately two-thirds of these additional deaths (47 000) were linked to disruptions in the provision of malaria prevention, diagnosis and treatment during the pandemic.
As in past years, the report provides an up-to-date assessment of the burden of malaria at global, regional and country levels. It tracks investments in malaria programmes and research as well as progress across all intervention areas. This latest report draws on data from 87 countries and territories with ongoing malaria transmission.
more

The World Health Organization (WHO) Global Status Report on Noncommunicable Diseases 2010 projects that noncommunicable diseases (NCDs) will be responsible for over 44 million deaths during the next decade, representing an increase of about 15% sinc
...
e 2010. Most of these deaths will occur in the WHO regions of Africa, South-East Asia and the Eastern Mediterranean. In the African Region alone, NCDs will cause around 3.9 million deaths by 2020.
more

The Policy Guidelines and Service Standards for National Sexual and Reproductive Health Programme document outlines the steps on how to offer and deliver services. Improving quality of care is critical to improving clients' health status as well as increasing
...
access to, and utilization of Sexual and Reproductive Health services. Service Standards and Guidelines are intended to be used by programme managers, implementers, trainers, surpervisors, and service providers as a tool for delivering quality care measures.
more
The EHSP in Botswana seeks to attain universal coverage of high-quality package of essential health services. The EHSP is an integrated collection of cost-effective interventions, promotive, preventive, curative, and rehabilitative, that address the main diseases, injuries and risk factors that affe
...
ct the population. The EHSP has two key purposes:
1) Provide a standardized package of basic services which forms the core of service delivery in all primary health care facilities
2) Promote a redistribution of health services by providing equitable access, especially in underserved areas, population, etc.
more

Measuring the Success of Family Planning Initiatives in Rwanda: A Multivariate Decomposition Analysis.
uhoza, Dieudonné Ndaruhuye, Pierre Claver Rutayisire, and Aline Umubyeyi.
Calverton, Maryland, USA: ICF International
(2013)
C2
DHS Working Papers No. 94 - This study described the family planning initiatives in Rwanda and analyzed the 2005 and 2010 RDHS data to identify factors that contribute to the increase in contraceptive use. The Blinder-Oaxaca technique was used to de
...
compose the contributions of women’s characteristics and their effects.
more

The Global Vaccine Action Plan (GVAP) 2011-2020, endorsed by Member States during the May 2012 World Health Assembly, has set ambitious targets to improve access to immunization and tackle vaccine-preventable diseases. This responsibility has been t
...
ranslated into firm commitments in February 2016, through the signature of the Addis Declaration on Immunization (ADI) by African Ministers and subsequently endorsed by the Heads of States from across Africa at the 28th African Union Summit held in January 2017. This commitment from the highest level of government comes as a catalyst to immunization efforts on the continent to deliver on the promise of universal immunization
more

This case study examines the humanitarian response to the conflict-related crisis in the North-East of Nigeria, focusing primarily on the period from 2015 to the end of 2016. The aim is test the central hypotheses of the Emergency Gap project: that the current structure, conceptual underpinning and
...
prevalent mindset of the international humanitarian system limits its capacity to be effective in response to conflict-related emergencies.
As with many conflict-related crises, the emergency in north-east Nigeria has deep and complex roots in the history of the region. The conflict began in 2009 and quickly developed beyond the control of the authorities. It unfolded in the midst of pre-existing political, social and economic tensions, making an effective humanitarian response exceedingly difficult. Despite this complexity, what is clear is that the crisis has resulted in a sprawling humanitarian disaster that has killed over 25,000 people as a direct result of the violence, and continues to devastate many more lives through hunger, psychological trauma and lack of access to healthcare. more
As with many conflict-related crises, the emergency in north-east Nigeria has deep and complex roots in the history of the region. The conflict began in 2009 and quickly developed beyond the control of the authorities. It unfolded in the midst of pre-existing political, social and economic tensions, making an effective humanitarian response exceedingly difficult. Despite this complexity, what is clear is that the crisis has resulted in a sprawling humanitarian disaster that has killed over 25,000 people as a direct result of the violence, and continues to devastate many more lives through hunger, psychological trauma and lack of access to healthcare. more
Due to the anticipated significant rise in VL testing occasioned by Ghana’s adaptation of 2016 ART guidelines, it has become necessary to develop this VL scale-up and operational plan to assure complete client access to laboratory monitoring towar
...
ds the achievement of the third 90 of the HIV care cascade. The plan will enhance VL testing, monitoring whilst improving the clinical and laboratory interface for improved client care.
more

Democratic dispensation in 1994 created a political and social platform that reshaped life in South Africa. There was a surge in common belief that the inequity and wrong of Apartheid should and could be rectified. Equity of access to water and sani
...
tation were obvious targets for improvement. In 1994, an estimated 14–15 million South Africans were without access to an improved water supply, while close to 21 million - more than half of the population at that time - did not have access to improved sanitation facilities. These problems were most severe in poorer rural areas. The water and sanitation sector became unified by the vision of universal access for all South Africans. This case study documents the progression of the sector between 1994 and 2016, and analyzes the impact of local systems created in South Africa to respond to the water and sanitation challenge.
more

Journal of the International AIDS Society 2017, vol. 20:e25026
In Myanmar, men who have sex with men (MSM) experience high risk of HIV infection. However, access to HIV testing and prevention services remains a challenge among this marginalized ... population. The objective of this study was to estimate population prevalence and correlates of prior HIV testing among young MSM (YMSM) and informs the development of HIV testing and intervention programmes that respond to the specific needs of this population.
https://doi.org/10.1002/jia2.25026 more
In Myanmar, men who have sex with men (MSM) experience high risk of HIV infection. However, access to HIV testing and prevention services remains a challenge among this marginalized ... population. The objective of this study was to estimate population prevalence and correlates of prior HIV testing among young MSM (YMSM) and informs the development of HIV testing and intervention programmes that respond to the specific needs of this population.
https://doi.org/10.1002/jia2.25026 more

Background Paper prepared for the 2015 Global Assessment Report on Disaster Risk Reduction
The aim of this paper is to help bring voluntary standards into the toolbox of disaster risk reduction, including both by encouraging their use by business and by enhancing their role in legislation and ... regulatory practice.
- Authorities can build awareness for standards in Disaster Risk Reduction (DRR), by facilitating access to relevant standards, encouraging education on DRR-related standards and involving the standardization community.
- Standards need to be sustained by a powerful infrastructure that allows for reliable inspections, audits and precise measurements to be conducted by skilled professionals.
- Risk management best practice needs to embed, as emdodies in standards, more fully in regulatory frameworks in sectors that are relevant. more
The aim of this paper is to help bring voluntary standards into the toolbox of disaster risk reduction, including both by encouraging their use by business and by enhancing their role in legislation and ... regulatory practice.
- Authorities can build awareness for standards in Disaster Risk Reduction (DRR), by facilitating access to relevant standards, encouraging education on DRR-related standards and involving the standardization community.
- Standards need to be sustained by a powerful infrastructure that allows for reliable inspections, audits and precise measurements to be conducted by skilled professionals.
- Risk management best practice needs to embed, as emdodies in standards, more fully in regulatory frameworks in sectors that are relevant. more

Rohingya Refugee Response Gender Analysis: Recognizing and responding to gender inequalities
Toma, Iulia; Chowdhury, Mita; Laiju, Mushfika; Gora, Nina; Padamada, Nicola
Oxfam, Action Against Hunger, Save the Children
(2018)
C1
This gender analysis was conducted to understand the different risks and vulnerabilities but also opportunities and skills for Rohingya and host community women, men, boys and girls. Data collection was conducted over three weeks from 8 April to 29 April 2018. The work aimed to identify the differen
...
t needs, concerns, risks and vulnerabilities of women, girls, boys and men in both Rohingya refugee communities and host communities in the Cox’s Bazar district of Bangladesh. The analysis shows various gaps in the humanitarian response for both communities, especially in terms of accountability, communication with affected communities and disaster preparedness, but also in equitable access to services, in particular for women and girls, and especially for the Rohingya community. The key findings are presented below, along with recommendations for action.
more

The National Health Plan (NHP) aims to strengthen the country’s health system and pave the way towards Universal Health Coverage (UHC),choosing a path that is explicitly pro-poor. The main goal of NHP 2017-2021 is to extend access to a Basic Essen
...
tial Package of Health Services (EPHS) to the entire population by 2020 while increasing financial protection.
more

The study analyses the current situation of children with disabilities in relation to realizing their rights and accessing basic services, as well as their life experiences in their communities. It also focuses on identifying the barriers created by society that prevent children with disabilities fr
...
om enjoying their human rights. This includes identifying negative attitudes; environmental and communication barriers; gaps in policies or their effective implementation.
The report reveals that children with disabilities in Myanmar are less likely to access services in health or education; rarely have their voices heard in society; and face daily discrimination as objects of pity. It also highlights how inadequate policies and legislation contribute to the challenges these children face.
The information available in this publication should be useful for policy makers, development partners and Disabled Persons Organisations to promote the realization of the rights of all children with disabilities. more
The report reveals that children with disabilities in Myanmar are less likely to access services in health or education; rarely have their voices heard in society; and face daily discrimination as objects of pity. It also highlights how inadequate policies and legislation contribute to the challenges these children face.
The information available in this publication should be useful for policy makers, development partners and Disabled Persons Organisations to promote the realization of the rights of all children with disabilities. more

The objectives of this guidance document are to:
1. Strengthen the capacity of country teams to effectively scale up and manage programmes to address severe acute malnutrition
2. Extend the geographic reach of quality treatment for SAM to all vulnerable communities in need
3. Maximize ... access to appropriate and quality treatment for SAM among all eligible children in the community at all times
4. Aid the formulation and implementation of national policies and strategies that support objectives 1 to 3
5. Aid the creation of an enabling environment that supports objectives 1 to 3 through advocacy, documentation of successful practices, support for operational research, mobilization of resources and collaboration with partners more
1. Strengthen the capacity of country teams to effectively scale up and manage programmes to address severe acute malnutrition
2. Extend the geographic reach of quality treatment for SAM to all vulnerable communities in need
3. Maximize ... access to appropriate and quality treatment for SAM among all eligible children in the community at all times
4. Aid the formulation and implementation of national policies and strategies that support objectives 1 to 3
5. Aid the creation of an enabling environment that supports objectives 1 to 3 through advocacy, documentation of successful practices, support for operational research, mobilization of resources and collaboration with partners more

Following the encouraging initial results of the pilot project, the Ministry of Health is committed to increasing access to MDR-TB diagnosis, treatment and care. An expansion plan for the programmatic management of drug-resistant TB has been develop
...
ed and forms part of the Five Year National Strategic Plan for TB Control, 2011-2015. The long-term goals of the MDR-TB expansion plan are threefold:
1. Diagnosis of MDR-TB in all groups of patients at risk for MDR-TB
2. Diagnosis of MDR-TB in all HIV-infected TB patients
3. MDR-TB treatment for all patients diagnosed with MDR-TB under WHO-endorsed treatment protocols more
1. Diagnosis of MDR-TB in all groups of patients at risk for MDR-TB
2. Diagnosis of MDR-TB in all HIV-infected TB patients
3. MDR-TB treatment for all patients diagnosed with MDR-TB under WHO-endorsed treatment protocols more

Climate change is a growing concern for Bangladesh because 90 percent of the country is approximately 10 feet above sea level. An evaluation was completed which discovered that high tides in Bangladesh were increasing 10 times more rapidly than the global average. This predicted rapid
...
increase in sea levels places Bangladesh four times higher than the global average. By 2050, approximately 20 percent of the inhabited land in Bangladesh will be inundated by the sea resulting in displacement for nearly 20 million people. The Government of Bangladesh has implemented policies and plans to focus on climate change concerns, but there is still much work to be completed.
Bangladesh is a nation which will continue to experience the devastating effects of climate change. These concerns for the nation are recognized and the Government of Bangladesh is working progressively to implement mitigation and preparedness measures along with making national economic and transportation improvements to better sever and protect the people of Bangladesh. more
Bangladesh is a nation which will continue to experience the devastating effects of climate change. These concerns for the nation are recognized and the Government of Bangladesh is working progressively to implement mitigation and preparedness measures along with making national economic and transportation improvements to better sever and protect the people of Bangladesh. more
The prevalence of chronic non-communicable diseases such as diabetes, cardiovascular diseases and cancers has been on the increase in Kenya in the recent past. This has been occasioned by changes in social and demogr
...
aphic situation in the country. The life expectancy in the country is improving, while the country is developing at a rapid pace. This has resulted in people living more years and at the time adopting lifestyles that have negative impacts on their health. This increase in diabetes and other non-communicable diseases has given rise to a double burden of communicable and non-communicable diseases in Kenya
more

Translation of the 1st ed., 2003
These guidelines were written for anyone trying to meet and solve the challenges of operating a warehouse today. They are an important reference tool for managers and staff, whether they are constructing a new warehouse, implementing a new warehouse syste ... m, or redesigning their current system.
Guidelines for Warehousing Health Commodities is for use by supply chain managers, logistics advisors, and warehouse managers who want to improve and increase efficiency in their current health commodity warehouse. more
These guidelines were written for anyone trying to meet and solve the challenges of operating a warehouse today. They are an important reference tool for managers and staff, whether they are constructing a new warehouse, implementing a new warehouse syste ... m, or redesigning their current system.
Guidelines for Warehousing Health Commodities is for use by supply chain managers, logistics advisors, and warehouse managers who want to improve and increase efficiency in their current health commodity warehouse. more

The purpose of the landscape analysis is ultimately to facilitate improved engagement of private providers, thereby contributing to universal access to quality and affordable TB care and the end of the TB epidemic. It focuses on the role of private
...
for-profit providers and on specific challenges and experiences in engaging them for TB prevention and care.
more
In 2017, 3.6 million of the estimated 10 million people with TB worldwide were “missed” by national TB programmes (NTPs). Two thirds of them are thought to access TB treatment of questionable quality from public and private providers who are not
...
engaged by the NTP. The quality of care provided in these settings is often not known or substandard. Closing these gaps and ensuring patient-centred care imply that quality-assured and affordable TB services must be made available wherever people choose to seek care.
more

The ASEAN Mental Health Systems Report
catalogues the situation of mental health in ASEAN
Member States. This report provides comprehensive
information on the progress made so far by AMS in
integrating mental health into national health systems,
increasing
...
access to care as well as challenges faced.
It also offers recommendations on how to improve the mental health system in
respective ASEAN Member States.
more

Treatment Improvement Protocol (TIP) Series No. 59
This Quick Guide is based entirely on information contained in TIP 59, published in 2014. No additional research has been conducted to update this topic since publication of TIP 59. | This Quick Guide provides succinct, easily accessible informatio
...
n to behavioral health administrators about developing culturally competent organizations. The guide is based entirely on Improving Cultural Competence, Number 59 in the Treatment Improvement Protocol (TIP) series. Users of the Quick Guide are invited to consult the primary source, TIP 59, for more information and a complete list of resources for improving cultural competence. To order a copy of TIP 59 or to access it online, see the inside back cover of this guide.
more

Stigma toward mental illness in Latin America and the Caribbean: a systematic review
Franco Mascayano, Thamara Tapia, Sara Schilling, Rubén Alvarado, Eric Tapia, Walter Lips, Lawrence H. Yang
Revista Brasileira de Psiquiatria
(2016)
CC
Stigma toward individuals with mental disorders has been studied extensively. In the case of
Latin America and the Caribbean, the past decade has been marked by a significant increase in
information on stigma toward mental illness, but these findi
...
ngs have yet to be applied to mental health services in Latin America. The objective of this study was to conduct a systematic review of studies relating to stigma toward mental illness in Latin America and the Caribbean. The authors specifically considered differences in this region as compared with manifestations reported in Western European countries
more

299 deaths have been recorded and 329 people are still missing, according to the Government.
• Latest assessments indicate that the homes of some tens of thousands of people have been destroyed or damaged beyond habitability. Most of these people are staying with hosts in the extended community.
...
• Revised Flash Appeal requires US$294 million to respond to the drought and Cyclone Idai.
• Food Cluster partners have so far assisted an estimated 30,000 people in the worst-affected areas of Chimanimani and Chipinge.
• Access to a sufficient quantity of water for drinking, cooking and personal hygiene has been restored for 43,000 people.
• Eight clusters have been activated to bolster the humanitarian response effort in support to the Government of Zimbabwe,
more

Barriers to the prompt and effective diagnosis and treatment of malaria exist at both the community and health facility level. Household surveys measure malaria case management at the population level with standard indicators that assess treatment-seeking behavior,
...
access to diagnostic testing, and access to appropriate treatment. Performance on these indicators varies widely from country to country. Among countries with Demographic and Health Surveys (DHS) or Malaria Indicator Surveys (MIS) completed between 2014 and 2016, advice and treatment was sought for a median of 47% of children under age 5 with fever.
more

These country reports provide information on the legal situation for displaced populations, namely asylum seekers, refugees, and returnees, where relevant, regarding access to mobile services, in each country covered

Yemen has already lost 2 decades of Human Development
The study warns of exponentially growing impacts of conflict on human development. It projects that if the war ends in 2022, development gains will have been set back by 26 years — almost a generation. If it continues through 2030, that setbac
...
k will increase to four decades.
Large File 35 MB!!!
more
Better Parenting Nigeria is a parenting education program whose goal is to see that families have the knowledge and skills needed to raise healthy, safe and resilient children. The program aims to ensure that:
The caregiver-child relationship is strengthened;
Caregiver capacity to understa
...
nd family needs and access resources and services is
increased; and
Caregiver capacity to protect children from all forms of harm and exploitation is
improved.
This Facilitator’s Manual is for the facilitator to use to support the community discussions, provide targeted messaging, and recommend suggestions for knowledge and experience sharing. It should be used hand-in-hand with the Community Discussion Guide.
more

Healthy Diets From Sustainable Food Systems. Summary Report of the EAT Lancet Commission
This report was prepared by EAT and is an adapted summary of the Commission Food in The Anthropocene: the EAT-Lancet Commission on Healthy Diets From Sustainable Food Systems.
To
...
access the EAT–Lancet Commission Hub page at The Lancet on the website https://www.thelancet.com/commissions/EAT
You can download the Summary Report in Arabic, Chinese, English, French, Indonesian, Portuguese, Russian and Spanish.
more

The mission of the Women’s Health Council is to inform and influence the development of health policy to ensure the maximum health and social gain for women in Ireland.
Its membership is representative of a wide range of expertise and interest in women’s health.
The Women’s Health Council
...
has five functions detailed in its Statutory Instruments:
1. Advising the Minister for Health and Children on all aspects of women’s health.
2. Assisting the development of national and regional policies
and strategies designed to increase health gain and social gain for women.
3. Developing expertise on women’s health within the health services.
4. Liaising with other relevant international bodies which have similar functions as the Council.
5. Advising other Government Ministers at their request.
more

This Toolkit aims to support the understanding and implementation of integrated mental health programs in humanitarian settings. It provides a framework for essential steps and components, with associated key guidance and resources, that strengthen the integration process, and is primarily intended
...
for (1) implementing agencies, but may also be useful for (2) donors, and (3) government actors. Users can access the three steps & three cross cutting components relevant to current program needs, or stages of programming.
Accessed August 7, 2019
more

According to official figures from Migración Colombia by the end of June 2019, there were more than 1.4 million Venezuelan refugees and migrants living in Colombia. The majority of people have settled in the border departments of La Guajira and Norte de Santander, continuing to cities along the Car
...
ibbean coast, or larger cities inland such as Medellin and Bogotá. Significant numbers of Venezuelans continue to cross Colombia by foot, heading for larger cities with more opportunities and better services or towards the southern border with Ecuador to continue their onward journey to a third country. Refugees and migrants arrive in Colombia with immediate humanitarian needs including access to safe accommodation, food, basic health care, but the prolonged nature of their displacement also requires longer term solutions including access to formal employment, education and social integration. The Interagency Group for Mixed Migration Flows (GIFMM) works closely with the Government at both the national level, and across 11 of the most affected departments, to deliver direct emergency assistance, protection, socio-economic integration activities and seeks to build the capacity of the host government.
more

For applying the new operational guidance on CB-MHPSS in the field, UNICEF country offices and partners will need ready access to tools and resources that can be used to implement the programs. By bringing together resources from different contexts,
...
the compendium makes options available to country offices and partners for programming.
The compendium aims to strengthen UNICEF capacity for MHPSS programming consistent with the IASC Guidelines for MHPSS in Emergencies and described by the 9 circles of support in the UNICEF operational framework.
The compendium is a compiled set of resources, already being used by UNICEF and partners, both national and international, in diverse settings.
more
Needs and barriers for mental health and psychosocial support among syrian refugees in lebanon: perspectives for future interventions
European Union Civil protection and Humanitarian Aid
European Union Civil protection and Humanitarian Aid
(2018)
CC
Results
Recommendations• NGOs should provide MHPSS services with a focus on empowerment and self-reliance
• Introduce interventions focusing on pain mechanisms, coping strategies and physical resilience
• Implement livelihood programmes
• Incre
...
ase service accessibility and outreach activities
• Provide support groups for people who have lost a close family member
• Highlight the importance of supervision and training
• Ensure high quality service provisions by applying relevant outcome measures and to further contribute to the evidence base for MHPSS
• Diversify MHPSS activities to different target groups, including men and women, and address the needs of elderly and individuals with disabilities
This study provides evidence of a large gap between the need of MHPSS among Syrian refugees and provided services. Of the 1082 respondents in this study, 62% expressed that they needed assistance to deal with physical pain and distress. Almost 80% reported being in pain, of which 27% were in severe or very severe pain. Additionally, 55% suffer from distress and 56% rate their own health as fair or poor. Even among the 18-25-yearolds, the prevalence of reporting their overall health as fair was 30.7%. For functionality levels, 28.5% felt severely or extremely emotionally affected by their health problems, and more than 20% had serious difficulties in doing day-to-day work. On the other hand, the majority (72-74%) had no problems in maintaining friendships and participating in community activities
more

HIV care in Central and Eastern Europe: How close are we to the target?
D. Gokengina,; C. Opreab; J. Begovacc; A. Horban; et al.
International Journal of Infectious Diseases; International Society for infectious Diseases ; Elsevier
(2018)
C2
International Journal of Infectious Diseases 70 (2018) 121–130
https://doi.org/10.1016/j.ijid.2018.03.007
1201-9712/© 2018 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases. This is an open access
...
article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
more

Compared to the previous five-year assessment period 2011–2015, the current five-year period 2015–2019 has seen a continued increase in carbon dioxide (CO2 ) emissions and an accelerated increase
...
in the atmospheric concentration of major greenhouse gases (GHGs), with growth rates nearly 20% higher. The increase in the oceanic CO2 concentration has increased the ocean’s acidity.
The five-year period 2015–20191 is likely to be the warmest of any equivalent period on record globally, with a 1.1 °C global temperature increase since the pre-industrial period and a 0.2 °C increase compared to the previous five-year period.
more

Survival of HIV patients with tuberculosis started on simultaneous or deferred HAART in the THRio cohort, Rio de Janeiro, Brazil
V. Saracenia; B. Durovnia; S. C. Cavalcante
Elsevier; The Brazilian Journal of Infectious Diseases; Science Direct
(2014)
C2
braz j infect dis. 2014;18(5):491–495
http://dx.doi.org/10.1016/j.bjid.2014.02.004
1413-8670/© 2014 Elsevier Editora Ltda. Este é um artigo Open Access sob a licença de CC BY-NC-ND

Clinical and epidemiological characteristics associated with unfavorable tuberculosis treatment outcomes in TB-HIV co-infected patients in Brazil: a hierarchical polytomous analysis
T. N. do Pradoa; J.t V. Rajand; A. E. Miranda; et al.
The Brazilian Journal of infectious diseases; Elsevier Editora Ltda.
(2016)
C2
braz j infect dis 2 0 1 7;2 1(2):162–170
http://dx.doi.org/10.1016/j.bjid.2016.11.006
1413-8670/© 2016 Sociedade Brasileira de Infectologia. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (htt
...
p://creativecommons.org/licenses/by-nc-nd/4.0/).
more

Policy brief. HIV testing services (HTS) and anti-retroviral therapy (ART) have been scaled up substantially. It is estimated that, globally, nearly 80% of people with HIV now know their status. With the offer of immediate ART initiation and improved treatment options,
...
access to and uptake of treatment have increased, too. Now, most people with HIV who know their status are obtaining treatment and care.
In response to these changes in the global HIV epidemic, WHO is encouraging countries to use three consecutive reactive tests for an HIV-positive diagnosis as their treatment-adjusted prevalence and national HTS positivity fall below 5% .
more
Public Health is the science field dedicated to promoting health and well-being, and preventing disease within the human population to ultimately increase the quality of our livelihood and life span. Public Health does not focus on individual patie
...
nts or diseases, but rather a given population and health system. The discipline is community-centered in its interventions and seeks to improve the health status of whole populations...
more

Previous crises, such as the Ebola virus disease (EVD) in West Africa in 2014, indicate the direct impact movement restrictions and disease containment efforts have on food availability, access, utilization and violence – particularly gender-based
...
violence (GBV). The importance of maintaining and upscaling food security interventions for the most vulnerable populations, alongside the health sector’s efforts to avert disease spread, is therefore undeniable. The COVID-19 outbreak in South Sudan threatens to paralyze an already fragile food system and negatively impact more than 6.5 million people in South Sudan who remain vulnerable. At the same time, the core national capacities for prevention, preparedness and response for public health events is limited, and the healthcare system has been weakened by years of conflict, poor governance and low investments.
more

A Review of Community Health Worker (CHW) knowledge, attitudes and practices relating to the sexual health of MSM, including existing training materials and manuals in Europe & neighbouring countries
C. Folch; P. Fernández-Dávila; J. Palacio-Vieira; et al.
European Commission; Centre d'Estudis Epidemiològics sobre les Infeccions de Transmissió Sexual i Sida de Catalunya (CEEISCAT); European AIDS Treatment Group
(2020)
C2
Accessed: 07.03.2020
A Review of Community Health Worker (CHW) knowledge, attitudes and practices relating to the sexual health of MSM, including existing training materials and manuals in Europe and neighbouring countries (D5.1)
Contract 2015 71 01 A behavioural survey for HIV/AIDS and assoc
...
iated infections and a survey and tailored training for community based health workers to facilitate access and improve the quality of prevention, diagnosis of HIV/AIDS, STI and viral hepatitis and health care services for men who have sex with men (MSM).
Pubic Health
more

Antibiotics have been a critical public health tool since the discovery of Penicillin in 1928, saving the lives of millions of people around the world. In developing country like ours, where the burden of treatable disease is very high and access to
...
health facilities and laboratories is difficult, antibiotics have long acted as miracle drugs. Today, however, the emergence of drug
resistance in bacteria is reversing the miracles of the past eighty years, with drug choices for the treatment of many bacterial infections becoming increasingly limited, expensive, and in some cases, nonexistent. Diseases previously regarded as relatively easy to manage are much harder to treat as doctors must use “last-resort” drugs that are more costly, take longer to work
and are often unavailable or unaffordable in developing countries. Moreover, regular prescription of antibiotics, random treatment, over the counter sales, inadequate dosage, inclusion of antibiotics in animal feeds and agriculture has contributed equally to emergence of antibiotics resistance as silent epidemic within the country.
more
The guidance provides critical considerations and practical checklists to keep schools safe. It also advises national and local authorities on how to adapt and implement emergency plans for educational facilities.
In the event of school closures, the guidance includes recommendations to mitigate
...
against the possible negative impacts on children’s learning and wellbeing. This means having solid plans in place to ensure the continuity of learning, including remote learning options such as online education strategies and radio broadcasts of academic content, and access to essential services for all children. These plans should also include necessary steps for the eventual safe reopening of schools.
Where schools remain open, and to make sure that children and their families remain protected and informed.
more
The Global Antibiotic Resistance Partnership (GARP)-Mozambique team, in partnership with the Center for Disease Dynamics, Economics & Policy (CDDEP), has produced this report as part of a solid com-mitment to develop actionable policy proposals to tackle antibiotic resistance and improve appropriate
...
antibiotic access. It is the result of a thorough review of published and unpublished data on antibiotic resistance and a long internal consultation effort that engaged academic scientists, health professionals and other stakeholders within Mozambique.
more
Putting Human Rights at the Heart of the Response
Topic in Focus: COVID-19 and Women’s Human Rights
15 April 2020
Stay-at-home restrictions and other measures restricting the movement of people contribute to an increase in genderbased violen
...
ce, a finding confirmed by media reports, official statements and information received from OHCHR field presences and human rights defenders in many countries.
Women and girls already in abusive situations are more exposed to increased control and restrictions by their abusers, with little or no recourse to seek support. Hotlines receive reports of women being threatened with being thrown out of their homes, exposed to the infection, or having financial resources and medical aid withheld.
more

Community engagement from a distance
Shongjog, the national platform for Communication with Communities in Bangladesh.
BBC Media Action
(2020)
C2
This short guide is designed to assist development and humanitarian agencies to think through how risk communication and community engagement activity related to Covid-19 can be carried out without face-to-face interaction with communities. By using remote methods, agencies will be able to safeguard
...
the health of their own and their partners’ staff and volunteers, while still ensuring that communities receive accurate, up-to-date information as well as having access to communication channels which allow them to provide feedback and share their concerns and worries.
more
The COVID-19 pandemic is causing untold fear and suffering for older people across the world. As of 26 April, the virus itself has already taken the lives of some 193,710 people, and fatality rates for those over 80 years of age is five times the global average. As the virus spreads rapidly to devel
...
oping countries, likely overwhelming health and social protection systems, the mortality rate for older persons could climb even higher.
Less visible but no less worrisome are the broader effects: health care denied for conditions unrelated to COVID-19; neglect and abuse in institutions and care facilities; an increase in poverty and unemployment; the dramatic impact on well-being and mental health; and the trauma of stigma and discrimination.
more
Psychological first aid (PFA) is a method of helping people in distress so they feel calm and supported to cope better with their challenges. It is a way of assisting someone to manage their situation and make informed decisions. The basis of psychological first aid is caring about the person in dis
...
tress and showing empathy. It involves paying attention to reactions, active listening and, if needed, practical assistance, such as problem solving, help to access basic needs or referring to further options for assistance. PFA helps normalize worry and other emotions, PFA also promotes healthy coping and provides feelings of safety, calming, and hope.
more

Three billion people – 40 per cent of the world’s population – do not have a place in their homes to wash their hands with water and soap. Three quarters of those who lack access to water and soap live in the world’s poorest countries and ar
...
e amongst the most vulnerable: children and families living in informal settlements, migrant and refugee camps, or in areas of active conflict. This puts an estimated 1 billion people at immediate risk of COVID-19 simply because they lack basic handwashing facilities.
The Hand Hygiene for All initiative aims to move the world towards this goal: supporting the most vulnerable communities with the means to protect their health and environment. It brings together international partners, national governments, public and private sectors, and civil society to ensure affordable products and services are available, especially in disadvantaged areas, and to enable a culture of hygiene.
more
Primary care health centers and providers who care for individuals with hypertension and cardiovascular disease have an important role to play in ensuring continued access to care, reducing the risk of coronavirus infection, and appropriately managi
...
ng people with these co-morbidities who acquire COVID-19. This guidance includes these considerations
more
This report outlines and analyses the implementation of the Bridge Builder Model. This is a two-way, capacity-sharing model aimed at bringing together local faith actors (LFAs) and international humanitarian actors to increase understanding, trust,
...
coordination and collaboration.
more

With the spread of the coronavirus (COVID-19) across Myanmar, many children and caregivers are required to stay in quarantine centres, in isolation and in hospitals, and special attention is needed to ensure children’s rights are protected in these settings. Violence, exploitation, abuse and negle
...
ct still occurs despite COVID-19 and continuity of the child protection case management system is essential to protect all children, including the most vulnerable. UNICEF’s Child Protection support focuses on mitigating the secondary impacts of physical distancing measures by ensuring children, parents and caregivers continue to have access to child protection services.
more
The COVID-19 pandemic has created challenges for forcibly displaced persons and the humanitarian organizations working to support them. With restrictions on movement and limited access to refugees, asylum-seekers, internally displaced persons (IDPs)
...
and stateless persons across the globe, UNHCR is supporting displaced communities to take the lead in the prevention of, and the response to, the existing and emerging protection needs of women, men, girls and boys of diverse backgrounds.
more

Remote Psychological First Aid during COVID-19 – May 2020
IFRC Reference Centre for Psychosocial Support
IFRC Reference Centre for Psychosocial Support
(2020)
CC
Psychological first aid (PFA) is a method of helping people in distress so they feel calm and supported to cope better with their challenges. It is a way of assisting someone to manage their situation and make informed decisions. The basis of psychological first aid is caring about the person in dis
...
tress and showing empathy. It involves paying attention to reactions, active listening and, if needed, practical assistance, such as problem solving, help to access basic needs or referring to further options for assistance. PFA helps normalize worry and other emotions, PFA also promotes healthy coping and provides feelings of safety, calming, and hope. These guidelines can be used by Red Cross Red Crescent National Societies to set up and run different kind of remote services for the public during the time of a COVID-19 response. It should be noted that the target group for the guidelines are adults.
more

Special Focus on COVID-19
The report provides updated estimates for drinking water, sanitation and hygiene in schools including progress from 2015 to 2019. It highlights the rapid improvement needed to ensure students have access to handwashing fac
...
ilities with soap and water during the COVID-19 pandemic, and to meet associated SDG targets by 2030.
more

As daily lives and communities are upended by COVID-19, concern is mounting that children’s exposure to violence may increase. Children with a history of abuse may find themselves even more vulnerable – both at home and online – and may experi
...
ence more frequent and severe acts of violence. Others may be victimized for the first time.
Understanding the current status of violence prevention and response services is therefore essential to assessing risks to children
more
Accessed on 20.10.2020
In its fight against maternal mortality, the government of Burkina Faso is supported
by the donor community which contributes to the health budget and also supports
specific projects aimed at improving access to health care
...
. This report acknowledges
the efforts to address maternal mortality undertaken by the government with the help
of the donor community, as well as projects led by international and national NGOs.
more
7. Rev Panam Salud Publica. 2020;44:e13
Haiti faces a double burden of disease. Infectious diseases continue to be an issue, while non-communicable diseases have become a significant burden of disease. More attention must also be focused on the increase
...
in worrying public health issues such as road injuries, exposure to forces of nature and HIV/AIDS in specific age groups. To address the burden of disease, sustained actions are needed to promote better health in Haiti and countries with similar challenges.
more

For the first time WHO and UNICEF bring together the data on sanitation coverage and investment, and how it impacts health, economies, and the environment. Citing evidence on what works from successful countries and global guidelines, WHO and UNICEF call for strong government leadership and investme
...
nt in resilient sanitation services. The report charts an ambitious way forward following the SDG6 global acceleration framework themes of governance, financing, capacity development, data and information, and innovation to achieve universal access to safe sanitation.
Read the full publication report here: https://www.who.int/publications/i/item/9789240014473.
more
Concentrations of the major greenhouse gases, CO2 , CH4 , and N2 O, continued to increase despite the temporary reduction in emissions in 2020 related to measures taken in response to COVID-19.
2020 was one of the three warmest years on record. T
...
he past six years, including 2020, have been the six warmest years on record. Temperatures reached 38.0 °C at Verkhoyansk, Russian Federation on 20 June, the highest recorded temperature anywhere north of the Arctic Circle.
The trend in sea-level rise is accelerating. In addition, ocean heat storage and acidification are increasing, diminishing the ocean’s capacity to moderate climate change.
more
14 January 2021
This practical guide can be used to help countries monitor and analyse the impact of COVID-19 on essential health services to inform planning and decision-making. It provides practical recommendations on how to use key performance indicators to analyse changes in
...
access to and delivery of essential health services within the context of the COVID-19 pandemic; how to visualize and interpret these data; and how to use the findings to guide modifications for safe delivery of services and transitioning towards restoration and recovery. The guide focuses on existing indicators and data that are captured in routine reporting systems and how they can be used by national and subnational authorities to understand specific contexts, challenges and bottlenecks. This guide supports Maintaining essential health services: operational guidance for the COVID-19 context, which provides an integrated framework to guide countries in their efforts to reorganize, adapt and maintain safe delivery of high-priority essential health services within the context of the pandemic.
more

This paper reviews the effects of vertical responses to COVID-19 on health systems, services, and people’s access to and use of them in LMICs, where historic and ongoing under-investments heighten vulnerability to a multiplicity of health threats.
...
We use the term ‘vertical response’ to describe decisions, measures and actions taken solely with the purpose of preventing and containing COVID-19, often without adequate consideration of how this affects the wider health system and pre-existing resource constraints.
more
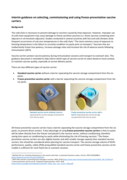
Interim Guidance, published 11 January 2021.
The cold chain is necessary to prevent damage to vaccines caused by heat exposure. However, improper use of cold chain equipment may cause damage to freeze-sensitive vaccines (i.e. those vaccines containing alum adjuvant or oil-emulsion adjuvant). Studie
...
s conducted in several countries with hot and cold climates show frequent occurrences of sub-zero temperatures in the cold chain. The most common cause of exposure to freezing temperature is the failure to correctly condition ice packs prior to transport. Vaccines that are inadvertently frozen lose potency, increase wastage rates and increase the risk of adverse events following immunization (AEFI). Vaccine carriers protect vaccine potency during immunization sessions and transport to outreach sites. This guidance document is intended to help inform which type of vaccine carrier to select based on local context, to maintain vaccine quality, especially at service delivery points.
more

Quality Assurance Framework for SARS-CoV-2 Antigen Rapid Testing for Diagnosis of COVID-19
recommended
ASLM in collaboration with the Africa Centres for Disease Control and Prevention, and in partnership with the Clinton Health Access Initiative, Amref and Last Mile Health present the Quality Assurance Framework for SARS-CoV-2 Antigen Rapid Testing f
...
or Diagnosis of COVID-19. This framework aims to provide general technical guidance to African Union Members States on the rollout, establishment, implementation, monitoring, and evaluation of SARS-CoV-2 Ag RDT interventions so as to effectively and efficiently detect, control and minimise errors in the performance of COVID-19 laboratory testing processes. It describes the core components for quality assurance, resources mobilisation and advocacy for scale up, monitoring, evaluation, learning and accountability for SARS-CoV-2 implementation.
more

Quality of care in fragile, conflict-affected and vulnerable settings: tools and resources compendium
recommended
This compendium represents a curated, pragmatic and non-prescriptive collection of tools and resources to support the implementation of interventions to improve quality of care in such contexts. Relevant tools and resources are listed under five areas: Ensuring
...
access and basic infrastructure for quality; shaping the system environment; reducing harm; improving clinical care; and engaging and empowering patients, families and communities.
more
Strategic communication is used to raise awareness of issues among specific target populations. It aims to provide timely, evidence-based, authoritative information and guidance needed for public health action. Proper implementation of strategic communication leads t
...
o sustained behaviour change and is essential in overcoming barriers to access to services or generating demand for such services.
more
This report describes findings from a telephone survey with 1,284 people conducted in February 2021. The survey examined how people respond to public health and social measures (PHSMs) to prevent COVID-19. The sample is representative of households with ac
...
cess to a landline or cell phone, but does not include people without access to phones. As phone penetration varies by country, findings should be interpreted with caution.
more

This report describes findings from a telephone survey with 1,328 people conducted in February 2021. The survey examined how people respond to public health and social measures (PHSMs) to prevent COVID-19. The sample is representative of households with ac
...
cess to a landline or cell phone, but does not include people without access to phones. As phone penetration varies by country, findings should be interpreted with caution.
more

This report describes findings from a telephone survey with 1,316 people conducted in February 2021. The survey examined how people respond to public health and social measures (PHSMs) to prevent COVID-19. The sample is representative of households with ac
...
cess to a landline or cell phone, but does not include people without access to phones. As phone penetration varies by country, findings should be interpreted with caution.
more
Preliminary overview of refugees and migrants self-reported impact of COVID-19
The study surveyed over 30,000 refugees and migrants living in 170 countries. Many of the respondents had fled war or dire economic conditions in their home country only to be faced with the additional challenges posed b
...
y COVID-19. Travel restrictions including border closures, suspension of resettlement travel, and last-minute deportation left many stranded or forced to stay in cramped, makeshift shelters or detention centers. Amid these uncertain, precarious conditions, many migrants described either a lack of access to health services or a fear of seeking them out — even if they were experiencing COVID-19 symptoms.
more
The regional Migrant Response Plan (MRP) for the Horn of Africa and Yemen includes urgent life-saving humanitarian and protection interventions to improve safe and dignified access to basic services for migrants and host communities while ensuring m
...
edium- to long-term actions aimed at addressing the drivers of migration.
more
COVID-19 Vaccines: 1 Safety Surveillance 2 Manual
While there is no indication that pregnant women have an increased susceptibility to infection with SARS-CoV-2, there is evidence that pregnancy may increase the risk of severe illness and mortality
...
from COVID-19 disease in comparison with non-pregnant women of reproductive age. As seen with non-pregnant women, a high proportion of pregnant women have asymptomatic SARS-CoV-2 infection and severe disease is associated with recognized medical (e.g., high body-mass index (BMI), diabetes, pre-existing pulmonary or cardiac conditions) and social (e.g., social deprivation, ethnicity) risk factors. Pregnant women with symptomatic COVID-19 appear to have an increased risk of intensive care unit admission, mechanical ventilation and death in comparison with non-pregnant women of reproductive age, although the absolute risks remain low. COVID-19 may increase the risk of preterm birth, compared with pregnant women without COVID-19, although the evidence is inconclusive.
more
This publication is based on the list of clinical interventions selected from clinical guidelines on prevention, screening, diagnosis, treatment, palliative care, monitoring and end of life care. This publication addresses medical devices for six types of cancer: breast, cervical, colorectal, leukem
...
ia, lung and prostate. The first section defines the global increase in cancer cases, the global goals to manage NCDs and the WHO activities related to these goals. The second section presents the methodology used for the selection of medical devices that support clinical interventions required to screen, diagnose, treat and monitor cancer stages, as well as the provision of palliative care, based on evidence-based information. The third section lists the priority medical devices required to manage cancer in seven different units of health care services: 1. Vaccination, clinical assessment and endoscopy, 2. Medical imaging and nuclear medicine, 3. Surgery, 4. Laboratory and pathology, 5. Radiotherapy, 6. Systemic therapy and 7. Palliative and end of life care
more

2021 UNAIDS Global AIDS Update. UNAIDS report shows that people living with HIV face a double jeopardy, HIV and COVID-19, while key populations and children continue to be left behind in access to HIV services

A Technical Brief for Breakthrough ACTION Field Teams
Social media can be used to collect and address rumors or popular beliefs among target audiences, share evidence-based and timely health information, receive instant feedback on materials, conduct remote trainings, promote awareness of a project
...
, its mission and events, and more. As increased numbers of people search online for health information, social media platforms are leading the lightning-speed spread of both dangerous coronavirus misinformation and the correct life-saving measures individuals, families, and communities can take to reduce their risk. Public health programs must have a proactive presence in these information-sharing spaces to provide access to trusted and accurate information.
more
This article looks at the Baseline Standards developed by the International Society for Paediatric
Oncology (SIOP) for paediatric oncology nursing care in low- and middle-income countries. The
Baseline Standards lay the foundation for effective care and address barriers such as inadequate
staffin
...
g levels, lack of support, limited access to nurse education and unsafe nursing environments.
more
Background Unrest in Chile over inequalities has underscored the need to improve public hospitals. Nursing has been overlooked as a solution to quality and access concerns, and nurse staffing is poor by international standards. Using Chile’s new d
...
iagnosis-related groups system and surveys of nurses and patients, we provide information to policy makers on feasibility, net costs, and estimated improved outcomes associated with increasing nursing resources in public hospitals.
more

New research exposes how women and children are disproportionally affected by climate migration, which puts them at greater risk of gender-based violence, child labour and exploitation.
Governments must ensure the safety and protection of women and girls in climate emergencies, including the safe
...
and equal access to basic services, food, and healthcare before, during, and after disasters. Women must also be included in decision making in their communities so they can lead on resilience building and address gendered issues of migration and displacement.
more
Early damage assessments indicate that at least 800,000 people could be directly exposed to minor to severe damages, including communication, access, security, loss of livelihoods, infrastructure, and health services could be impacted.
This inter-agency guidance document aims to supplement the COVAX demand creation package for COVID-19 vaccines with key considerations for humanitarian contexts and marginalized populations with specific access and communication needs.
21 Sept.2021
...
more
24 Nov. 2021
Action against gender-based violence being pushed to the outlying margins of the global COVID-19 response
A new Oxfam report shows an undeniable increase in gender-based violence (GBV) during the COVID-19 pandemic around the world t
...
o which too many governments and donors are not doing enough to tackle.
The report, The Ignored Pandemic: The Dual Crisis of Gender-Based Violence and COVID-19, showed the number of calls made by survivors to domestic violence hotlines in ten countries during the first months of lockdown. The data reveals a 25 – 111 percentage surge; in Argentina (25%), Colombia (79%), Tunisia (43%), China (50%), Somalia (50%), South Africa (69%), UK (25%), Cyprus (39%), Italy (73%) and the largest increase in Malaysia where calls surged by over 111%.
more
This Global Competency Standards sets the benchmark for the health workforce in providing equality of care to refugees and migrants. Refugee and migrant populations are highly diverse, with significant variation in life experiences, health needs and access
...
to health care. The standards described outline expected behaviours of health workers in delivering quality care to refugees and migrants and can be used to inform the outcomes of education programmes aligned with standards for care. The Competency Standards is designed to provide a foundation to support the development of competency-based curricula tailored to the local context and for health workers to achieve a minimum level of competence. The importance of person-centred, culturally responsive care is emphasized in the nine competency standards, which recognize the need for health workers to be trained, supported and empowered within strong health systems
more
COVID-19 vaccine hesitancy is currently one of the main obstacles to worldwide herd immunity and socioeconomic recovery. Because vaccine coverage can vary between and within countries, it is important
to identify sources of variation so that policies can be tailored to different population groups.
...
In this paper, we analyze the results from a survey designed and implemented in order to identify early adopters and
laggers in six big cities of Latin America. We find that trust in government and science, accurate knowledge about the value of vaccination and vaccine effects, perceived risk of getting sick, and being a student
increase the odds to get vaccinated. We also identify potential laggers as women and populations between 20 and 35 years old who are not students. We discuss specific strategies to promote vaccination among
these populations groups as well as more general strategies designed to gain trust. These findings are specific to the context of Latin America insofar as the underlying factors associated with the choice to be
vaccinated vary significantly by location and in relation to individual-level factors.
more
Round 3: Key informant findings from 129 countries, territories and areas - Quarter 4 2021
Countries reported disruptions in all health-care settings. In more than half of countries surveyed, many people are still unable to access care at the prima
...
ry care and community care levels. Significant disruptions have also been reported in emergency care, particularly concerning given the impact on people with urgent health needs. Thirty-six per cent of countries reported disruptions to ambulance services; 32% to 24-hour emergency room services; and 23% to emergency surgeries.
Elective surgeries have also been disrupted in 59% of countries, which can have accumulating consequences on health and well-being as the pandemic continues. Disruptions to rehabilitative care and palliative care were also reported in around half of the countries surveyed.
Major barriers to health service recovery include pre-existing health systems issues which have been exacerbated by the pandemic as well as decreased demand for care.
more

Six months after the earthquake, World Vision's efforts have made it possible to provide emergency assistance to selected beneficiaries among the most vulnerable through the distribution of food and hygiene kits and to address the psychosocial needs of children, adolescents, and young people deprive
...
d of classrooms. During this recovery phase of the response by World Vision teams have been focusing on rebuilding and rehabilitating school infrastructure in order to facilitate the return to school in safer conditions given the almost permanent seismic risks. Six months later, the security situation continues to deteriorate with an increase in kidnappings and nationwide strikes to protest against the rising insecurity.
more