Filter
1935
Text search:
ca
Featured
158
361
Language
Document type
1013
422
264
90
38
37
29
20
9
8
3
1
1
Countries
144
61
56
56
43
39
33
31
31
27
24
22
21
20
17
16
16
14
13
13
13
13
13
13
13
13
13
13
12
12
12
12
11
11
11
10
10
10
9
8
8
7
7
7
7
7
7
7
6
5
5
5
5
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
550
154
107
73
39
22
18
Toolboxes
234
193
181
147
121
103
65
52
52
51
51
45
28
27
22
20
12
11
10
10
7
7
5
Version 02, veröffentlicht am 23.12.2020
The guide is organized into the major types of toxicities, the associated symp-toms, possible offending medications, and the suggested nursing assessments and interventions. Some symptoms (e.g. nausea) may be associated with a num-ber of underlying causes and may be mild, or a symptom of
...

Recommendations for the adaptation of Emergency Medical Teams (EMTs) at temporary sites for COVID-19 vaccination. Draft Version 2.3, November 2021
Auswertung der Befragungen in ausgewählten Unterkünften
22. Februar 2021
Das Epidemiologische Bulletin 8/2021 beschreibt die Chancen, aber auch Risiken und Limitationen bei der Eigenanwendung von Antigen-Selbsttests zum Nachweis einer akuten Infektion mit SARS-CoV-2.
WHO-2019-nCoV-genomic_sequencing

Orientaciones provisionales 16 de diciembre de 2020
En el presente documento se resumen las orientaciones actuales de la OMS para la vigilancia de salud pública en relación con la coronavirosis de 2019 (COVID-19) en el ser humano debida a la infección por el coronavirus del síndrome respiratori
...
Jährlicher Bericht des Deutschen Forums für Kriminalprävention (DFK) mit einem Beitrag zum Gewaltschutz in Flüchtlingsunterkünften

: interim guidance, 17 February 2021
This document provides interim guidance on the management of the blood supply in response to the pandemic outbreak of coronavirus disease (COVID-19). It emphasizes the importance of being prepared and responding quickly and outlines key actions and measures that
...

29 Dec 2021. Comprehensive slideset updated regularly to include the latest data and guidance on best practices for COVID-19 diagnosis and prevention of COVID-19 transmission.
Ziel dieser qualitativen Studie ist eine Situationsanalyse der Regelungen und Maßnahmen auf lokaler Ebene, die zur Prävention und Eindämmung der SARSCoV-2-Ausbreitung in SU für Geflüchtete ergriffen wurden.
В целом считается, что люди, страдающие астмой (ЛСА), подвергаются повышенному риску при респираторных
инфекциях, что ежегодно подтверждается во время в�
...

People with asthma (PWA) generally are considered at higher risk from respiratory infections, as is seen annually with influenza. At the outset of the COVID-19 pandemic, PWA were widely assumed to be at increased risk from COVID-19. However, as data emerged throughout 2020, the association between a
...
The Guidelines on promotive and preventive mental health interventions for adolescents - Helping Adolescents thrive (HAT), provide evidence-informed recommendations on psychosocial interventions to promote mental health, prevent mental disorders, and reduce self-harm and other risk behaviours among
...

The Guidelines on promotive and preventive mental health interventions for adolescents - Helping Adolescents thrive (HAT), provide evidence-informed recommendations on psychosocial interventions to promote mental health, prevent mental disorders, and reduce self-harm and other risk behaviours among
...

Despite some improvements, current levels of air pollution still pose a considerable risk to the environment and to human health in the WHO European Region. One issue of concern is that monitoring of particulate matter is very limited in the countries of eastern Europe, the Caucasus and central Asia
...
Objetivos.
Estimar la carga de tuberculosis (TB) en menores de 15 años y describir las características clínico, epidemiológicas y los resultados del tratamiento antituberculoso en Ecuador.
Métodos.
Se realizó un estudio retrospectivo utilizando los datos del programa nacional de TB de los
...

Клиническое определение случая состояния после COVID-19 методом дельфийского консенсуса, 6 октября 2021 г.
recommended
WHO has developed a clinical case definition of post COVID-19 condition by Delphi methodology that includes 12 domains, available for use in all settings. This first version was developed by patients, researchers and others, representing all WHO regions, with the understanding that the definition ma
...
The Lancet , A comment
Oct 6, 2021. Entschlossene Solidarität oder endlose Krise.
Vortrag für: Tag der Forschung und Beratung der kath. Universität von Misiones (UCAMI), Argentinien


Buku Pegangan -Panduan penilaian dan alur layanan berbasis individu di layanan kesehatan primer
recommended
Indonesian Version of: Integrated care for older people (ICOPE): guidance for person-centred assessment and pathways in primary care. The ICOPE guidance for person-centred assessment and pathways in primary care (ICOPE Handbook) helps community health and care workers put the recommendations o
...
The COVID-19 pandemic has led to large increases in healthcare waste, straining under resourced healthcare facilities and exacerbating environmental impacts from solid waste. This report quantifies the additional COVID-19 healthcare waste generated, describes current healthcare waste management syst
...
Lecture 9 Developing countries regional anesthesia lecture series

Ziel der Psychiatrieberichterstattung ist eine umfassende und transparente Darstellung der Situation sowie das Aufzeigen von Veränderungsbedarfen der psychiatrischen, psychotherapeutischen, psychosomatischen und psychosozialen Versorgung in Bayern. Ab Seite 59 wird auf die Situation von Menschen mi
...
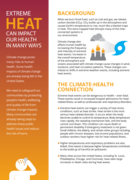
Climate change also affects human health by increasing the frequency and intensity of extreme heat events. Increases in
the overall temperature of the atmosphere and oceans associated with climate change cause changes in wind, moisture, and heat circulation patterns. These changes contribute to shi
...
M. Zaman et al. (eds.), Measuring Emission of Agricultural Greenhouse Gases
and Developing Mitigation Options using Nuclear and Related Techniques,
https://doi.org/10.1007/978-3-030-55396-8_

Cardiovascular disease, diabetes, chronic obstructive pulmonary disease, cancers, and other non-communicable diseases are among the leading causes of morbidity and mortality in low-income, middle-income, and high-income countries, and The Lancet Taskforce recently made the case for investing in non-
...
Tuberculosis (TB) is an infectious disease that usually affects the lungs, though it can affect any organ in the body. It can develop when bacteria spread through droplets in the air. TB can be fatal, but in many cases, TB is preventable and treatable. This report examines the human rights impact of
...
The Lancet Global Health Volume 9, ISSUE 3, e361-e365, March 01, 2021
The public health community has tried for decades to show, through evidence-based research, that safe water, sanitation, and hygiene (WASH) and clean cooking fuels that reduce household air pollution are essential to safeguard he
...
Die Klimakrise stellt die größte Bedrohung der menschlichen Gesundheit im21. Jahrhundert dar. Die mit ihr
einhergehenden Umweltveränderungen, die unter anderem zu Hitzewellen, Überflutungen und Unterernährung durch
Ernährungsunsicherheit führen, wirken sich bereits heute negativ auf die Ge
...
Epidemiologisches Bulletin 15/2022 p.21-23

The American Journal of Tropical Medicine and Hygiene Volume 106: Issue 1 p.12-14.he piece highlights a body of research that suggests tiny plastic particles could disrupt immune and endocrine systems, damage organs, and cause other health problems. “Without a fundamental reimagining of global
...
Die Studie untersucht auf Basis von Daten des Mikrozensus sowie des SVR Integrationsbarometers den Stand der Integration von (Spät) Aussiedlerinnen und (Spät)Aussiedlern in Deutschland in zahlreichen Lebensbereichen

Ethnic disparities in COVID-19 persist, with increased rates of infection, severe disease, and death among people from minority ethnic groups. COVID-19 vaccination rates also remain lowest in these communities compared with white people in the UK. Among people older than 18 years, the proportion who
...
J Bras Pneumol. 2022;48(2):e20220082
The spread of Severe Acute Respiratory Syndrome - Coronavirus 2 (SARS-CoV-2) continues to progress, causing damage in several countries of the world due to its rapid transmissibility and significant mortality rates, despite government measures to contain its tra
...

On average across 34 countries, more than half of all adults surveyed (56%) say climate change has already had a severe effect in the area where they live. More than seven in ten (71%), including a majority in every single country, expect climate change will have a severe effect in their area over t
...

FGM = Female Genital Mutilation

Trachoma is one of the 17 WHO-defined Neglected Tropical Diseases
(NTDs) that affect over 1 billion of the world’s poorest and most
marginalized people. It is caused by the bacterium chlamydia trachomatis.
Snakebite envenoming is a potentially life-threatening disease that typically results from the injection of a mixture of different toxins (“venom”) following the bite of a venomous snake. Envenoming can also be caused by venom being sprayed into a person’s eyes by certain species of snakes tha
...
Between 2012 and 2016, development assistance for HIV/AIDS decreased by 20·0%; domestic financing is therefore critical to sustaining the response to HIV/AIDS. To understand whether domestic resources could fill the financing gaps created by declines in development assistance, we aimed to track spe
...
The document, "Progress on the Prevention and Control of Non-Communicable Diseases," reports on global efforts to reduce the impact of NCDs, such as heart disease, cancer, diabetes, and chronic respiratory diseases, following the commitments made at high-level United Nations meetings. It highlights
...
Злоупотребление алкоголем и алкоголизм относятся к ведущим причинам ухудшения здоровья и повышения смертности населения. Чрезмерное употребление алкоголя служи
...

In many countries neonatal tetanus is responsible for half of all neonatal deaths due to vaccine-preventable diseases and for almost 14% of al¡ infant deaths. It is estimated that in the 1970s more than 10,000 newborns died annually from neonatal tetanus in the Americas. Neonatal tetanus is prevent
...
These guidelines deal specifically with water, sanitation and hygiene, and are designed to be used in schools in low-cost settings in low- and medium-resource countries to:
• assess prevailing situations and plan for required improvements;
• develop and reach essential safety standards as a f
...


Septìeme Édition 2019
The present book deals not only with emergency response, but also with measures designed to reduce the impact of disasters on environmental health infrastructure, such as water supply and sanitation facilities. It also aims to strengthen the ability of people to withstand the disruption of their acc
...

• provide scientific information on the safety, efficacy, and quality control/ quality assurance of widely used medicinal plants, in order to facilitate their appropriate use in Member States;
• provide models to assist Member States in developing their own mono- graphs or formularies for these
...
• provide scientific information on the safety, efficacy, and quality control/ quality assurance of widely used medicinal plants, in order to facilitate their appropriate use in Member States;
• provide models to assist Member States in developing their own mono- graphs or formularies for these
...

• provide scientific information on the safety, efficacy, and quality control/ quality assurance of widely used medicinal plants, in order to facilitate their appropriate use in Member States;
• provide models to assist Member States in developing their own mono- graphs or formularies for these
...

WHO Model Formulary for Children
recommended
WHO Model Formulary for children based on the Second Model List of Essential Medicines for Children 2009.
In 2007, the World Health Assembly passed a Resolution titled ‘Better Medicines for Children’. This resolution recognized the need for research and development into medicines for children,
...

HIV & AIDS Treatment in Practice No. 188

The 7th edition of the Orange Guide provides practical guidance to health workers on the front line of TB control. It includes sections on HIV, MDR-TB and a review of the recommended treatment regimens
2nd edition

Handbook of Foodborne Pathogenic Microorganisms and Natural Toxins


New edition
A Global Inventory of Alternative Medical Waste Treatment Technologies

Dermatological Preparations For The Tropics
recommended
A formulary of dermatological preparations and background information on therapeutic choices, production and dispensing. 2nd edition

Assessing Mental Health and Psychosocial Needs and Resources Toolkit For Humanitarian Settings
recommended
Available in different languages: English, French, Arabic, Russian


Report of a World Health Organization and International Diabetes Federation meeting



Rreport of a WHO Consultative Meeting Kolkata India 2012
A review of policy and practice; zero Hunger Phase 1

Bulletin of the World Health Organization Volume 91, Number 4, April 2013, 237-312
This manual provides guidance for policymakers on the issue of prehospital trauma care systems. The main areas covered include the organisation of the prehospital trauma care system, capacity development, data collection, transportation and communication, as well as ethical and legal considerations
...
Undernutrition increases the risk of tuberculosis (TB) and in turn TB can lead to malnutrition. Undernutrition is therefore highly prevalent among people with TB. It has been demonstrated that undernutrition is a risk factor for progression from TB infection to active TB disease and that undernutrit
...



Volume 1 covers emergency triage assessment and treatment, and acute care for a severely ill or acutely injured patient for approximately the first 24 hours of care. It describes the clinical procedures commonly used in emergency and acute care, and gives a summary of the medicines used and the step
...



A training manual for safe motherhood action groups (MAMaZ)

- The Role of Plant Nutrition in Supporting Food Security
- Micronutrient Malnutrition: Causes, Prevalence, Consequences and Interventions
- Fertilizer Application and Nutraceutical Content in
Health-Functional Foods
- Plant Nutrition and Health Risks Associated with Plant Diseases
- Human Heal
...

Provide guidance to HIV care practitioners on the optimal use of antiretroviral (ARV) agents for the treatment of HIV infection in adults and adolescents.

Advancing Health, Learning and Equity through WASH in Schools

The Baby-friendly Hospital Initiative (BFHI) is a global effort launched by WHO and UNICEF to implement practices that protect, promote and support breastfeeding. It was launched in 1991 in response to the Innocenti Declaration. The global BFHI materials have been revised, updated and expanded for i
...

6th edition

En los últimos 30 años los eventos adversos en la región de la Comunidad Andina ocasionaron la muerte de unas 227.000 personas, y pérdidas por cerca de 12.000 millones de dólares. Ecuador vivió una situación similar. El objetivo de este manual es propiciar una ade
...


Educational materials (slide presentations) from FAO covering important biosecurity aspects in poultry farms