Filter
1822
Text search:
Cardiovascular
Disease
Featured
183
375
Language
Document type
791
446
291
87
68
65
31
12
8
6
6
5
4
1
1
Countries
148
102
48
45
43
37
31
29
27
27
27
21
20
19
19
19
18
17
17
16
16
15
15
14
13
13
13
13
12
12
12
12
12
10
10
9
9
8
8
8
8
8
8
7
7
6
6
5
5
5
5
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
715
273
201
58
46
29
6
1
Toolboxes
284
207
172
110
62
53
45
43
32
32
28
21
21
18
17
8
7
7
5
4
3
3
2
Hypertension is the number one health related risk factor in India, with the largest contribution to burden of disease and mortality. It contributes to an estimated 1.6 million deaths, due to ischemic heart
...
The article "Air Pollution: The Emergence of a Major Global Health Risk Factor" discusses the significant health impacts of air pollution, a leading risk factor for global mortality. It highlights the adverse effects of fine particulate matter (PM2.5) and tropospheric ozone, linking them to
...
The Noncommunicable Diseases Country Profiles 2018 by the World Health Organization (WHO) provides an in-depth look at the burden of noncommunicable diseases (NCDs) such as cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes
...
WHO Package of Essential NCD interventions will help to improve the coverage of appropriate services for people with NCDs services in primary care settings. The HEARTS technical package provides a strategic approach to improving cardiovascular healt
...
The webpage from the Pan American Health Organization (PAHO) focuses on the significant health impacts of air pollution in the Americas. It explains how exposure to air pollutants contributes to various health issues, including respiratory and cardiovascul
...
The webpage from the Institute for Health Metrics and Evaluation (IHME) provides an analysis of air pollution as a significant global health risk. It details how air pollution contributes to severe health problems, including respiratory diseases and increased mortality rates. The site explains diffe
...
Non-communicable diseases (NCDs) are major global public health concerns that cause nearly three-quarters of the burden of mortality worldwide. Cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes alone account for over eight
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The World Health Organization (WHO) fact sheet on ambient (outdoor) air quality and health highlights the significant health risks posed by outdoor air pollution. It reports that in 2019, ambient air pollution was responsible for approximately 4.2 million premature deaths globally, primarily due to
...
The Our World in Data webpage on air pollution provides an extensive overview of the global impact of air pollution on health and the environment. It presents data on sources of pollution, such as industry, vehicles, and domestic energy use, and highlights the associated health risks, including resp
...
WHO list of priority medical devices for management of cardiovascular diseases and diabetes
recommended
This publication was developed in response to the need for a reference list of priority medical devices required for management of noncommunicable diseases (NCDs), focusing on cardiovascular diseases and diabetes, especially for low- and middle-inco
...

A short Guide for Health Practitioners
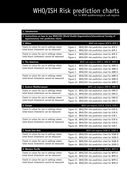
There are two sets of charts. One set (14 charts) can be used in settings where blood cholesterol can be measured. The other set (14 charts) is for settings in which blood cholesterol cannot be measured. Both sets are available in colour and shades of black on a compact disc. Each chart can only be
...

The volume presents data on the surgical burden of disease, disability, congenital anomalies, and trauma, along with health impact and economic analyses of procedures, platforms, and packages to improve care in settings with severe budget limitation
...
The substantial burden of death and disability that results from interpersonal violence, road traffic injuries, unintentional injuries, occupational health risks, air pollution, climate change, and inadequate water and sanitation falls disproportionally on low- and middle-income countries. Injury Pr
...

This study aimed to estimate the proportion of Mozambicans eligible for pharmacological treatment for hypertension according to single risk factor and total cardiovascular risk approaches. It concluded that a total of 19.8% of 40–64-year-olds woul
...
These guidelines for the prevention and management of cardiovascular diseases are a critical ingredient for streamlining care across the entire health services provision continuum. They are a strategic component in achieving unive
...
Hypertension is referred to as a “silent killer”. Most people with hypertension are unaware of their condition as in most cases, they experience no warning signs or symptoms hence they are not identified or treated. Hypertention is associated with a number of conditions, disability, and causes o
...
The substantial burden of death and disability that results from interpersonal violence, road traffic injuries, unintentional injuries, occupational health risks, air pollution, climate change, and inadequate water and sanitation falls disproportionally on low- and middle-income countries. Injury Pr
...

Topics in Antiviral Medicine 25 Issue 2 May/June 2017
Accessed February 6, 2020
Palliative care has been shown to provide significant and diverse benefits for patients with serious, complex,or life-limiting health problem.
Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R., editors. Disease Control Prio
...
While there has been real progress in addressing the burden of disease in the WHO African region, the COVID-19 pandemic has highlighted the link between health, economics and security, as the region saw decades of progress threatened, including posi
...

The main message emerging from this new comprehensive global assessment is that premature death and disease can be prevented through healthier environments – and to a significant degree. Analysing the latest data on the environment-
...
Diabetes is a serious, chronic disease that occurs either when the pancreas does not produce enough insulin (a hormone that regulates blood sugar, or glucose), or when the body cannot effectively use the insulin it produces. Diabetes is an important
...

Effective implementation of WHO PEN, combined with other very cost effective population-wide interventions, will help even resource constrained settings to attain the global voluntary targets related to reduction of premature mortality and preventionof heart attacks and strokes.

BMC Family Practice201415:165, DOI: 10.1186/1471-2296-15-165
Open Access

As the culminating volume in the DCP3 series, volume 9 will provide an overview of DCP3 findings and methods, a summary of messages and substantive lessons to be taken from DCP3, and a further discussion of cross-cutting and synthesizing topics across the first eight volumes. The introductory chapte
...

Infectious diseases are the leading cause of death globally, particularly among children and young adults. The spread of new pathogens and the threat of antimicrobial resistance pose particular challenges in combating these diseases. Major Infectious Diseases identifies feasible, cost-effective pack
...

Includes a Special Report on the Financial and Personal Benefits of Early Diagnosis
2018 Alzheimer’s Disease Facts and Figures is a statistical resource for U.S. data related to Alzheimer’s disease
...

Noncommunicable diseases (NCDs) are the principal cause of morbidity, disability and premature mortality in Azerbaijan. The most effective way to reduce the NCD burden is to prevent NCD development, by addressing thebehavioural risk factors underlying NCDs at the population and individual leve
...
The COVID-19 pandemic has impacted regular cardiovascular healthcare access and delivery. Service utilisation has declined, and excess cardiovascular mortality has been reported in several countries
...
Glob Heart . 2020 Oct 13;15(1):69. doi: 10.5334/gh.891.

The Regional Action Framework for Noncommunicable Disease Prevention and Control provides a unified vision of objectives and recommended actions to combat the noncommunicable disease (NCD) epi
...


Lancet Oncol 2018 Published Online September 12, 2018 http://dx.doi.org/10.1016/S1470-2045(18)30447-9
Calls for greater implementation research (IR) capacity came in the wake of compelling evidence that implementation strategies are critically important for the dissemination and facilitation of evidence-informed policies and interventions to tackle noncommunicable diseases (NCDs), thereby improving
...
Published OnlineJuly 14, 2021https://doi.org/10.1016/S2214-109X(21)00164-9. New Lancet research offers the first comprehensive analysis of the growing footprint of noncommunicable and injury-related neurological disorders to India’s overall disease
...
The Lancet. 13 March 2022. doi: 10.1016/S0140-6736(21)02868-3. Previous Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) studies have reported
national health estimates for Ethiopia. Substantial regional variations in socioeconomic status, population, demography, and access to hea
...

Case definitions, clinical classification, and disease phases Dengue, Chikungunya, and Zika
recommended
A person who lives in or has traveled in the previous 14 days to areas with dengue transmission, and presents with acute fever that has typically lasted 2 to 7 days, and two or more of the following clinical manifestations: nausea or vomiting, exanthema, headache or retro-orbital pain, myalgia or ar
...
The document "Global Report on Diabetes" by the World Health Organization (WHO) provides an in-depth analysis of diabetes as a global health challenge. It covers the rising prevalence of the disease, the associated risk factors, and the increasing b
...
The purpose of this document is to present concise information on the current case definitions for dengue, chikungunya, and Zika proposed by PAHO, as well as information on the clinical phases and severity classification of dengue and chikungunya.


Large File: 85 MB!!!. Please download directly from the website link

Lancet Glob Health 2018 Published Online September 12, 2018 http://dx.doi.org/10.1016/S2214-109X(18)30409-1

20 February 2013
Update on 2004 Background Paper (Written by Saloni Tanna)
Priority Medicines for Europe and the World "A Public Health Approach to Innovation"
Rev Saude Publica. 2022; 56: 22.
Published online 2022 Apr 11. doi: 10.11606/s1518-8787.2022056004040
Air pollution is a major environmental risk factor and contributor to chronic, noncommunicable diseases (NCDs). However, most public health approaches to NCD prevention focus on behavioural and biomedical risk factors, rather than environmental risk factors such as air pollution. This article discus
...
Guidance for health workers

The document is intended to facilitate the detection, evaluation and management of incident EVD cases in Germany. It primarily addresses public health service staff and health care workers in hospitals, outpatient clinics and emergency services in Germany. It is a work in progress, intended to evolv
...



Lancet Glob Health 2018, Published Online September 12, 2018 http://dx.doi.org/10.1016/S2214-109X(18)30387-5
This booklet provides an overview of all findings from the Global Burden of Disease 2017 study. Published in The Lancet in November 2018, GBD 2017 provides for the first time an independent estimation of population, for each of 195 countries and ter
...
A all for global Action. The Oral Health Atlas. Second edition
7. Rev Panam Salud Publica. 2020;44:e13
Haiti faces a double burden of disease. Infectious diseases continue to be an issue, while non-communicable diseases have become a significant burden of disease
...

This report provides a review and analysis of the research landscape for three diseases – Chagas disease, human African trypanosomiasis and leishmaniasis – that disproportionately afflict poor and remote populations with limited access to health
...
The Global Burden of Disease Study (GBD) began 30 years ago with the goal of providing timely, valid and relevant assessments of critical health outcomes. Over this period, the GBD has become progressively more granular. The latest iteration provide
...
MMWR Morbidity and Mortality Weekly Report December 19, 2014 / 63(50);1205-1206

Together we can Prevent and Control the World's Most Common Diseases
Objectives of the training manual
(1) To improve knowledge of NCD trends, burdens, as well as systems for management and monitoring of NCD services for Township Medical Officers (TMOs), Township Public Health Officers (TP ...
Objectives of the training manual
(1) To improve knowledge of NCD trends, burdens, as well as systems for management and monitoring of NCD services for Township Medical Officers (TMOs), Township Public Health Officers (TP ...
16-24 February 2020

The WHO continuously reviews available data on SARS-CoV-2 variants of concern. For this version, the global epidemiological
situation of the COVID-19 pandemic as of 21 January 2022 – at a time when the Omicron VOC had been identified in 171
countries across all six WHO Regions and was rapidly re
...

This manual provides a framework for morbidity management and disability prevention of patients affected by NIDs and gives specific guidance for the proper care of patients suffering from chronic conditions caused by lymphatic filariasis, leprosy, trachoma, and Chagas
...

This manual provides a framework for morbidity management and disability prevention of patients affected by NIDs and gives specific guidance for the proper care of patients suffering from chronic conditions caused by lymphatic filariasis, leprosy, trachoma, and Chagas
...
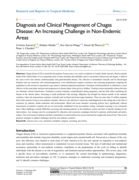
Research and Reports in Tropical Medicine 2022:13 25–40.
Chagas disease (CD) is caused by the parasite Trypanosoma cruzi, and it is endemic in Central, South America, Mexico and the South of the United States. It is an important cause of early mo
...
The Pharmaceutical Forum of the Americas (PFA) has previously published guidelines and organised campaigns for community pharmacists on the prevention, detection and control of arbovirus infections in 2018 with a grant from the FIP Foundation for Pharmacy Education and Research. Building on that exp
...

Ghana Med J. 2012 Jun;46(2 Suppl):69-78.

The evidence base for differentiated care for stable patients has grown in recent years. There has been less attention, however, to developing differentiated models of care for patients with advanced or unstable HIV disease. Current clinical guideli
...

Infection prevention and control in the context of coronavirus disease (COVID-19): A living guideline
recommended
This second edition of the Infection prevention and control in the context of coronavirus disease (COVID-19): A living guideline provides the most up to date technical guidance on mask use in community settings in the context of COVID-19.
In thi
...

Lancet Public health 2022 January 6, 2022 https://doi.org/10.1016/ S2468-2667(21)00249-8
Growth in the number of individuals living with dementia underscores the need for public health planning efforts and policy to address the needs of this group. Country-level estimates can be used to inform nati
...

Not long ago, on the occasion of the 100th anniversary of the discovery of Chagas disease, several campaigns denounced the scant progress has been made in diffrent spheres- medical, scientific and politcal- but major challanges still remain. This is
...
Background: Community health worker (CHW) programmes are a valuable component of primary care in resource-poor settings. The evidence supporting their effectiveness generally shows improvements in disease-specific outcomes relative to the absence of
...

The mounting burden of type 2 diabetes is a major concern in healthcare systems worldwide. The purpose of this study is to investigate the trend of type 2 diabetes from 1990 to 2019 in Asia.

It summarizes guidance on how to manage – and when to refer – children and adolescents presenting with common complaints and conditions. It includes information to enable primary health care providers to coordinate the continued care of children and adolescents with long-term conditions and dise
...
Enfoque de riesgo para la prevención de enfermedades cardiovasculares, consenso 2014
Climate change also affects human health by increasing the frequency and intensity of extreme heat events. Increases in
the overall temperature of the atmosphere and oceans associated with climate change cause changes in wind, moisture, and heat circulation patterns. These changes contribute to shi
...

Acute Radiation Syndrome (ARS) (sometimes known as radiation toxicity or radiation sickness) is an acute illness caused by irradiation of the entire body (or most of the body) by a high dose of penetrating radiation in a very short period of time (usually a matter of minutes). The major cause of thi
...
Acute Radiation Syndrome (ARS) (sometimes known as radiation
toxicity or radiation sickness) is an acute illness caused by
irradiation of the entire body (or most of the body) by a high dose
of penetrating radiation in a very short period of time (usually
...

Evaluation and Diagnosis of Penicillin Allergy for Healthcare Professionals
The Public Health Burden of Commercial Tobacco Use
The burden of disease and death from commercial tobacco* use in the United States is
overwhelmingly caused by cigarettes and other combustible tobacco products.

Public Health and the Environment | Geneva 2009

Progress towards targets of the Global action plan on dementia

A summary of health effects, resources, and adaptation examples from health departments funded by CDC’s Climate and Health Program
The document provides the NICE Quality Standard for managing Type 2 diabetes in adults (QS209). It outlines evidence-based recommendations for preventing Type 2 diabetes, structured education, continuous glucose monitoring (CGM), medication such as SGLT2 inhibitors, and regular care processes to mon
...