Filter
8089
Text search:
J.
Featured
Recommendations
595
New Publications
1562
Language
English
5942
Spanish
740
French
677
Russian
361
Portuguese
343
German
220
Arabic
167
Indonesian
65
Nepali
58
Chinese
55
Ukrainian
30
Farsi
18
Turkish
15
Hindi
12
Burmese
11
Italian
10
Romanian
10
Greek
10
Kurdish
10
Swahili
9
Serbian
9
Vietnamese
9
Albanian
7
Dari
7
Urdu
6
Pashto
6
Georgian
6
Tigrinya
5
Polish
5
Japanese
5
Kreyol
4
Bengali
4
Tamil
4
Hausa
3
Somali
3
Amharic
3
Malay
3
Thai
3
Bulgarian
3
Hungarian
3
Local Languages 2
2
Afrikaans
2
Kannada
2
Korean
2
Swedish
2
Dutch
2
Slovenian
2
Estonian
2
Danish
2
Lithuanian
2
Persian
2
Macedonian
2
Ndebele
1
Tagalog
1
Croatian
1
Finnish
1
Czech
1
Slovakian
1
Punjabi
1
Gujarati
1
Bosnian
1
Armenian
1
Chuukese
1
Hebrew
1
Mirpuri
1
Belarusian
1
Document type
No document type
4183
Studies & Reports
1686
Guidelines
1175
Manuals
381
Fact sheets
210
Strategic & Response Plan
198
Training Material
122
Situation Updates
44
Infographics
28
Resource Platforms
23
Brochures
19
Videos
13
Online Courses
4
Dashboards/Maps
2
App
1
Countries / Regions
Global
312
India
253
Brazil
186
Latin America and the Carribbean
177
South Africa
157
Western and Central Europe
154
Germany
152
Kenya
146
Nepal
138
Russia
133
Africa
120
Mozambique
102
Ethiopia
100
Liberia
94
Nigeria
93
Ukraine
91
Indonesia
89
Sierra Leone
85
Congo, Democratic Republic of
85
Uganda
85
Malawi
83
Rwanda
82
Senegal
77
Tanzania
71
Eastern Europe
71
Burkina Faso
67
Zambia
66
Myanmar / Burma
65
Venezuela
63
Syria
60
Colombia
58
Paraguay
58
Bangladesh
57
Ghana
52
Argentina
52
Middle East and North Africa
51
Asia
46
Cameroon
45
Haiti
45
Philippines
44
Angola
43
Zimbabwe
42
Benin
41
Guinea
40
West and Central Africa
38
Peru
37
South–East Asia Region
35
Eastern Europe and Central Asia
35
Yemen
33
South Sudan
31
Chile
31
East and Southern Africa
30
Ecuador
28
Guinea-Bissau
26
Lesotho
26
Mali
25
Namibia
25
Cambodia
23
Bolivia
21
Côte d’Ivoire / Ivory Coast
19
Sudan
18
USA
17
Botswana
17
El Salvador
17
Madagascar
17
Spain
17
Thailand
15
China
14
Pakistan
13
Afghanistan
13
Lebanon
13
Western Pacific Region
13
Iraq
12
Tajikistan
12
Jordan
11
Portugal
11
Somalia
10
Eswatini/ Swaziland
10
Albania
10
Vietnam
10
Chad
9
Sri Lanka
9
Georgia
9
Niger
8
Central African Republic
8
Mexico
8
Italy
8
Southern Africa
8
Kyrgyzstan
8
North America
8
Saudi Arabia
7
Honduras
7
North Macedonia
6
Guatemala
6
Jamaica
6
France
6
Morocco
5
Turkey
5
Egypt
5
Libya
5
Nicaragua
5
Congo-Brazzaville
5
Estonia
5
Moldova
5
Iran
5
Kazakhstan
5
United Kingdom
5
Belarus
5
Togo
4
Palestine
4
Armenia
4
Laos
4
Canada
4
Uruguay
4
Japan
4
Tunisia
4
Malaysia
3
Papua New Guinea
3
Dominican Republic
3
Switzerland
3
Hungary
3
Burundi
3
Mongolia
3
Timor Leste/ East Timor
3
Qatar
3
Israel
3
Cuba
2
Greece
2
Poland
2
North Korea
2
Romania
2
Bosnia and Herzegovina
2
Gambia
1
Mauritania
1
Singapore
1
Vanuatu
1
Austria
1
Serbia
1
Other region
1
Solomon Islands
1
Bhutan
1
Djibouti
1
Lithuania
1
Slovakia
1
Australia
1
Turkmenistan
1
Denmark
1
Belgium
1
Norway
1
Latvia
1
Authors & Publishers
World Health Organization WHO
864
et al.
517
World Health Organization
364
World Health Organization (WHO)
201
World Health Organisation (WHO)
179
IACAPAP
139
UNICEF
115
UNAIDS
108
WHO
104
USAID
93
Pan American Health Organisation PAHO
68
Organización Mundial de la Salud OMS
52
PLoS ONE
49
World Health Organization WHO, Regional Office of Europe
46
Stop TB Partnership
44
Organisation Mondiale de la Santé OMS
41
UN Children's Fund UNICEF
41
Organisation Mondiale de la Santé OMS
38
Pan American Health Organization (PAHO)
37
Pan American Health Organization PAHO
37
ICF International
35
CDC
32
UNFPA
31
UNOPS
29
END TB
28
Disability, CBR & Inclusive Development Journal (DCIDJ)
27
ICAP
27
The Lancet
27
Ministry of Health & Family Welfare, India
26
Organisation mondiale de la Santé
26
European Centre for Disease Prevention and Control
25
Ministerio de Salud Argentina
25
Organización Panamericana de la Salud
25
OPAS
24
PEPFAR
24
African Union
23
Ministry of Health, Kenya
23
World Health Organization (Europe)
23
Pan American Health Organization PAHO, World Health Organization WHO
22
Robert-Koch-Institut RKI
22
Africa CDC Centres for Disease Control and Prevention
21
Oxfam
21
University Teaching Hospital, et al.
21
Centers for Disease Control and Prevention CDC
20
Pan American Health Organization
20
UNDP
19
BMJ Global Health
18
Centers for Disease Control and Prevention
18
EngenderHealth
18
European Centre for Disease Prevention and Control ECDC
18
Organisation mondiale de la Santé (OMS)
18
Federal Ministry of Health, Nigeria
17
PLoS Medicine
17
PLoS Neglected Tropical Diseases
17
BioMed Central
16
Every Preemie—SCALE
16
Indian Council of Medical Research (ICMR)
16
World Health Organization WHO, Regional Office of Africa
16
International Union Against Tuberculosis and Lung Disease
15
Organización Mundial de la Salud
15
World Bank
15
Ministry of Health and Social Welfare, Tanzania
14
Organização Mundial da Saúde (OMS)
14
World Health Organization Europe
14
Всемирная организация здравоохранения
14
European Monitoring Centre for Drugs and Drug Addiction
13
Government of Nepal, Ministry of Health and Population
13
Ministerio de Salud, Peru
13
Ministry of Health, Zambia
13
Save the Children
13
United Nations Children's Fund (UNICEF)
13
Human Resources for Health
12
International Association for Child and Adolescent Psychiatry and Allied Professions
12
MINISTÉRIO DA SAÚDE, Brasil
12
BMC Public Health
11
Elsevier
11
FG Consulting Group
11
Food and Agriculture Organization of the United Nations FAO
11
IASC Reference Group on Mental Health and Psychosocial Support in Emergency Settings
11
International Union Against Tuberculosis and Lung Disease, World Health Organization
11
PAHO
11
UNAIDS (Joint United Nations Programme on HIV/AIDS)
11
UNHCR
11
C. Smyth, et al.
10
Catholic Relief Services CRS
10
Cochrane Library
10
et al
10
International federation of nurse anesthetics
10
International Federation of Red Cross and Red Crescent Societies
10
Ministerio de Salud Pública de Ecuador
10
Ministry of Health
10
Ministry of Health and Social Services (MOHSS)
10
Ministry of Health, Rwanda
10
National Department of Health South Africa
10
The World Bank
10
United Nations Division for Social Policy Development (DSPD) & United Nations Department of Economic and Social Affairs (DESA)
10
C. Daniels
9
European Centre for Disease Prevention and Control ECDC
9
Global Task Force on Cholera Control (GTFCC)
9
Government of Nepal
9
Hesperian
9
Human Rights Watch
9
Indonesian Urological Association
9
Ministry of Health & Social Welfare India
9
Ministry of Health and Social Welfare, Liberia
9
Ministry of Health Republic of Indonesia
9
Ministry of Health, Malawi
9
National Health Mission
9
PubMed.gov
9
Rüppel, J.
9
The International Federation of Red Cross and Red Crescent Societies IFRC
9
World Health Organization (Americas)
9
Всемирная организация здравоохранения (ВОЗ)
9
Avert
8
BMC Health Services Research
8
BMJ Open
8
Brakarsh, J.
8
Catholic Health Association of India (CHAI), Misereor
8
Dept. of Health, Republic of South Africa
8
Government of Malawi, Ministry of Health
8
ICRC
8
IFRC
8
Jhpiego
8
Journal of the International AIDS Society
8
L. Steinitz
8
Médecins sans Frontières
8
Ministerio da Saude, Brasilia
8
Ministerio de Salud El Salvador
8
Ministerio de sanidad - España
8
Ministry of Health, Ghana
8
National AIDS
8
OCHA Services
8
PMC
8
World Bank Group
8
Саратовский научно-медицинский журнал
8
ALNAP
7
Bimberg, L.
7
BMC
7
BMC Infectious Diseases
7
Catholic Relief Services
7
Centers for Disease Control and Prevention (CDC)
7
Centre for Health & Infectious Disease Research
7
European Centre for Disease Prevention and Control (ECDC)
7
Indonesian Heart Association
7
International Confideration of Midwives
7
International Federation of Red Cross And Red Crescent Societies IFRC
7
International Journal of Infectious Diseases
7
J. M. Rey
7
Kamps, B.S.
7
mhGAP
7
Ministry of Health and Family Welfare, Government of India
7
Ministry of Health, Republic of Uganda
7
National Library of Medicine
7
ONUSIDA
7
Ovid
7
PubMed
7
Regional Office for Africa
7
The Lancet Global Health
7
United Nations Office on Drugs and Crime
7
World Health Organization (WHO), Regional Office for South-East Asia
7
World Health Organisation
7
World Health Organization (WHO) & The World Bank (WB)
7
World Health Organization WHO, Regional Office for Europe
7
AidData at William & Mary
6
AIDSinfo
6
Bulletin of the World Health Organization
6
Christoffel-Blindenmission (CBM)
6
Cordner, S.
6
D. Raben
6
European Union
6
G. Ayala
6
Global Heart
6
Hartmann-Boyce J., N. Lindson
6
Indian Council of Medical Research
6
International Panel on Climate Change IPCC
6
J. Gardemann and A.M. Buschmann
6
JAIDS Journal of Acquired Immune Deficiency Syndromes
6
Kenya Ministry of Health
6
Lancet Migration
6
Malaria Consortium
6
Ministerio da Saude Brasilia
6
Ministerio de Salud Chile
6
Ministère de la Santé Publique et de la Population, Haiti
6
Ministry of Health Nepal
6
Ministry of Health, Government of Nepal
6
Myanmar Red Cross Society
6
OECD
6
OPAS, OMS
6
OPS
6
Organisation de la Santé Mondiale
6
Pan African Medical Journal
6
Pan American Health Organization (PAHO), OPS
6
President of the Republic of Indonesia
6
R. Coninx
6
Republic of Kenya, Ministry of Health
6
The Independent Panel
6
Tribuna del Investigador
6
UNITAID
6
World Health Organization WHO
6
World Health Organization (WHO), Regional Office for South-East-Asia
6
World Health Organization WHO, UNICEF
6
World Health Organization, Regional Office for Africa
6
World Heart Federation
6
World Meteorological Organization
6
World Vision
6
Africa Center for Disease Control and Prevention
5
AOSIS
5
Asian Disaster Preparedness Center, Tsunami Global Lessons Learned Project
5
bmj
5
BMJ Journals
5
Bousquet, J.
5
C. Daniels, et al.
5
Centro de Coordinación de Alertasy Emergencias Sanitarias
5
Christoffel Blinden Mission (CBM)
5
Department of Health, Republic of South Africa
5
et. al.
5
Food and Agriculture Organization of the United Nations
5
Frontiers in Public Health
5
GIZ
5
Global Polio Eradication Initiative GPEI
5
Health Policy Project
5
Hindawi
5
ICF
5
Inter-Agency Standing Committee IASC
5
Inter-agency Working Group on Reproductive Health in Crises
5
International Centre for Evidence in Disability (ICED)
5
International Journal of Mental Health Systems
5
J.
5
J. Bear
5
J. Butler
5
Lancet
5
M. Alonso González
5
M. Smelyanskaya, J. Duncan (The Focus Group Consulting)
5
MEDBOX
5
Médecins sans Frontières (MSF)
5
Médecins sans Frontières MSF
5
Ministerio de Salud Bolivia
5
Ministerio de Salud de Peru
5
Ministère de la Santé Publique, République Démocratique du Congo
5
Ministry of Health and Social Welfare, National AIDS Control Programme, Tanzania
5
Ministry of Health and Social Welfare, The United Republic of Tanzania
5
Ministry of Health Ghana
5
Ministry of Health of Republic of Indonesia
5
Ministry of Health, Nepal
5
Ministry of Health, Uganda
5
National AIDS Control Organization (NACO), Ministry of Health and Family Welfare, Government of India
5
Organización Mundial de la Salud (Américas)
5
Organização Mundial da Saùde
5
Organização Mundial da Saúde
5
Organização Pan-Americana da Saúde
5
Pan American Journal of Public Health
5
PRONASIDA
5
Regional Office for Europe
5
Research Gate
5
Rev Panam Salud Publica
5
Social Science in Humanitarian Action: A Communication for Development Platform
5
The Global Fund
5
The Union
5
UN High Commissioner for Refugees UNHCR
5
UN-Habitat
5
UNAIDS (Joint United Nations Programme on HIV/AIDS)
5
United States Agency for International Development
5
WHO Regional Office for Africa
5
World Health Organisation WHO
5
ВОЗ
5
Министерство здравоохранения Российской Федерации
5
A. Armstrong
4
A. Tareen
4
A. von Gontard
4
Africa CDC
4
Africa Centres for Disease Control and Prevention Center for Disease Dynamics, Economics & Policy
4
Alabí Montoya, F.J.
4
and C. Hoffmann
4
and J. Mauder
4
Bernard van Leer Foundation
4
BMC Medicine
4
Bundesamt für Migration und Flüchtlinge BAMF
4
C.G. Alvarenga Cardoza, K.M. Díaz de Naves
4
Cambridge University Press
4
care
4
CBM
4
Centers for Diseases Control and Prevention
4
Children & Aids
4
Clinical Infectious Diseases
4
CoreGroup
4
D. Adams
4
Dirección de Control de Enfermedades Inmunoprevenibles
4
E. Garralda
4
EADAP
4
Eastern Mediterranean Region
4
European Centers for Disease Control and Prevention ECDC
4
European Commission
4
FHI360
4
FIGO
4
Ghana AIDS Commission
4
Global Health: Science and Practice
4
Government of India, Central Tuberculosis Division, Ministry of Health and Family Welfare
4
Government of India, Ministry of Health and Family Welfare, National AIDS Control Organisation (NACO)
4
Handicap International, CBM
4
Health Policy and Planning
4
IAS
4
International Council of Nurses
4
ISPO
4
J Acquir Immune Defic Syndr
4
J. Byrne
4
J.-J. Kim
4
Journal of Global Health
4
K. Munir
4
Kementerian Kesehatan Republik Indonesia
4
London School of Hygiene and Tropical Medicine
4
London School of Hygiene and Tropical Medicine (LSHTM)
4
M. B. Mello
4
Masekela, R.
4
MEDBOX Team
4
METAdrasi
4
Ministerio de Salud
4
Ministerio de Salud y Protección Social Bogotá, Colombia
4
Ministerio de Salud, Gobierno de Chile
4
Ministério da saúde
4
Ministry of Health and Population, Health service Department.
4
National Department of Health, Republic of South Africa
4
O. Fiertag
4
OCHA
4
OCHA Services Reliefweb
4
OMS
4
Organización Mundial de Saude and OPAS
4
Organização Mundial da Saúde (Américas)
4
Organizaición Mundial de la Salud
4
PAHO (Pan American Health Organization
4
PAHO/World Health Organization
4
Plan
4
Plan International
4
PRONASIDA, et al.
4
Pub Med
4
Quinn, V., and A. Guyon
4
Reliefweb
4
ResearchGate
4
Rockville, Maryland, USA: ICF International
4
Rüppel J.
4
Rüppel T.
4
S. F. Jakobsen
4
SIAPS
4
Swiss Agency for Developoment and Coperation SDC
4
The Republic of the Union of Myanmar, Ministry of Health and Sports
4
The Republic of the Union of Myanmar, Relief and Resettlement Department
4
UKaid
4
UN Office for the Coordination of Humanitarian Affairs
4
UN Women
4
UNESCO
4
UNHCR Greece
4
UNODC
4
USAID, et al.
4
Wolters Kluwer Health
4
Word Health Organization
4
World Federation for Mental Health (WFMH)
4
World Health Organization (Western Pacific Region)
4
World Health Organization (WHO), Regional Office for South-East Asia
4
World Health Organization)
4
World Health Organization, Europe
4
World Health Organization, Regional Office for Europe
4
World Health Organization, Regional Office for the Americas
4
A. Aerts, M. Grzemska
3
A. Berg
3
A. Bone
3
A. Latypov
3
A. Martin
3
A. Sönnerborg
3
A. Turkova
3
African Palliative Care Association
3
Alan J. Flisher, Michelle Funk, Natalie Drew et al.
3
Annals of Global Health
3
Asociación Colombiana de Infectiologiá ACIN
3
Avances Cardiol
3
Ärzte der Welt
3
Baatiema L. et al.
3
Bozorgmehr, K.
3
BPtK Bundespsychotherapeuten Kammer
3
British Medical Journal
3
BUKO Pharma-Kampagne
3
Bull World Health Organ
3
Bundesministerium der Justiz und für Verbraucherschutz
3
Bundeszentrale für gesundheitliche Aufklärung
3
Butenop, J.
3
C. Carandang
3
C. Gray
3
C. Hamelmann
3
C.-C. Hung
3
Child Health Division, Ministry of Health and Social Welfare, Government of India
3
Chimbari, M.J.
3
Clinical Care Options
3
Clinical Pocket Reference
3
Colombia. Ministerio de Salud y Protección Social
3
Community Health Impact Coalition
3
Conant, J.
3
Conseil international des Infirmières (CII)
3
CoPEH Canada
3
Cure Americas
3
D.
3
D. A. Enarson, S. M. Kennedy, D. L. Miller, et al.
3
D. Mark
3
D. Sculier
3
De Brouwere V., Zinnen V., Delvaux T.
3
DeZIM Institut
3
DHS
3
Dieleman J.
3
Dunn, M.
3
ECRI
3
Elsevier Ltd
3
European Respiratory Journal
3
European Union EU
3
F. Çuhadaroğlu-Çetin
3
F. D. Zepf
3
Fadem, P.
3
Federal Ministry of Health Nigeria
3
Federal Ministry of Health, Ethiopia
3
FIND
3
Flood, D.
3
Forsyth, C.
3
G. Sander
3
Global Health Action
3
Global Laboratory Initiative
3
Global Mental Health
3
Government of Nepal, Nepal Nutrition and Food Security Portal
3
Government of Rwanda
3
H. Getahun
3
H. Marval-Ospino
3
Harm Reduction International
3
Health and Human Rights Journal
3
Health Research Policy and Systems
3
Help Age International
3
Holy Father Paul VI
3
ICF International, et al.
3
ILEP
3
ILEP International Federation of Anti-Leprosy Associations
3
INTECH
3
Inter-Agency Standing Committee IASC, et al.
3
InterAction, The Rockefeller Foundation
3
International Committee of the Red Cross (ICRC)
3
International Health
3
International League Against Epilepsy (UK Chapter) and Epilepsy Society
3
International Organization for Migration IOM
3
International Pharmaceutical Federation (FIP)
3
International Rescue Committee
3
Iris (Institutional Repository)
3
J. Fuentes
3
J. Hamilton
3
J. Klinte
3
J. Liu
3
J. Morris
3
J. Watts Belser, D. David
3
J.-G. Kühling
3
J.F.Oletta L.
3
JICA
3
Jiyan Foundation for Human Rights
3
K. Ciceri
3
Kamala Achu, Kathy Al Jubah, Svein Brodtkorb, et al.
3
Kangmennaang J.
3
Kirkuk Center for Torture Victims and Dulwich Centre Foundation International
3
L. Cailhol
3
L. Gicquel
3
L. Nyblade
3
Leonard Cheshire Disability and Inclusive Development Centre
3
Libreria Editrice Vaticana
3
Malaria Journal
3
Malteser International
3
Management Sciences for Health
3
Mauder, S.
3
Maxwell, J.
3
McCullagh S, Hunter B, Houle K et al.
3
MEASURE Evaluation
3
Medecins Sans Frontiers
3
Medical Mission Institute
3
Medicines Control Authority of Zimbabwe (MCAZ)
3
Menteri Kesehatan Republik Indonesia
3
Ministerio de la Protección Social, Colombia
3
Ministerio de Salud Pública del Ecuador
3
Ministerio de Salud Pública y Bienestar Social
3
Ministerio de Salud Pública y Bienestar Social Paraguay
3
Ministerio de Salud Pública y Bienestar Social Paraguay: Organización Panamericana de la Salud, et al.
3
Ministerio de Salud Pública, Paraguay
3
Ministerio de Salud, Bogota, Colombia
3
Ministère de la Santè et de la Prévention, Senegal Programme National de Lutte contre le SIDA
3
Ministère de la Santé Publique, Republique Démocratique du Congo
3
Ministério da Saúde Brasil
3
Ministério da Saúde Secretaria de Vigilância em Saúde, Brazil
3
Ministério da Saúde, Secretaria de Atenção Primária à Saúde Brasil
3
Ministry of Health & Social Welfare, Liberia
3
Ministry of Health and Child Welfare, Zimbabwe
3
Ministry of Health and Family Welfare Government of India
3
Ministry of Health and Sanitation Sierra Leone
3
Ministry of Health, Botswana
3
Ministry of Health, Gabarone, Botswana
3
Ministry of Health, Zambia, et al.
3
MSMGF
3
Myanmar Climate Change Alliance (MCCA)
3
N. Chkhartishvili
3
NACO
3
National Agency for the Control of AIDS (NACA)
3
National Department of Health, South Africa
3
National HIV
3
National Institute of Statistics of Rwanda (NISR)
3
National Institute of Statistics of Rwanda (NISR), the African Institute for Development Policy (AFIDEP) and UNFPA
3
Nations Unies
3
Nature Communications
3
NDoH South Africa
3
Nepal Ministry of Health and Population, New ERA, and ICF International
3
npj Primary Care Respiratory Medicine
3
OCCHA Services
3
Oranizatión Panamerica de la Salud
3
Organisation Mondiale de la Santé, Bureau régional de l'OMS pour l'Afrique
3
P. Gomes de Alvarenga
3
P. J. de Vries
3
Pan American Health Organisation PAHO, OPS
3
Parasites and Vectors
3
Pata Pata Pata
3
Patel P.
3
Philippine Society for Microbiology and Infectious Diseases
3
Physicians for Human Rights
3
PLoS Med
3
Population Council
3
Pretoria University Law Press (PULP)
3
Pusat Krisis Kesehatan
3
Quality Rights
3
R. Baggaley
3
R. M. Rapee
3
R. R. Althoff
3
ReAct
3
Registered Nurses’ Association of Ontario (RNAO)
3
Results for Development (R4D)
3
Robert Koch Institut
3
Robert-Koch-Institut
3
Rockström, J.
3
Rockville, Maryland, USA: ICF
3
Routledge
3
Rüppel, T.
3
Rwanda Biomedical Center - Institute of HIV
3
S. Gupta
3
S. Mares
3
S. Taylor
3
Saratov Journal of Medical Scientific Research
3
Schweizerisches Rotes Kreuz
3
Science Direct
3
Seiglie, J.A.
3
Silba A.
3
Social Science in Humanitarian Action
3
Springer International Publishing
3
T. Lempp
3
T. T. Bella-Awusah
3
The Center for Disease Dynamics, Economics & Policy CDDEP
3
The DHS Program
3
The Global Fund To fight AIDS, Tuberculosis and Malaria
3
The Indonesian Association of Pulmonologist
3
The Lancet Planetary Health
3
The National Child Traumatic Stress Network (NCTSN)
3
The Republic of the Union of Myanmar
3
The Sphere Project
3
Three Millennium Development Goal Fund (3MDG)
3
Treatment Action Group
3
U.S. Global Change Research Program
3
UN Enivronemnt Programme UNEP
3
UNICEF, et al.
3
United Nations
3
United Nations Children’s Fund (UNICEF)
3
United Nations Office on Drug and Crime UNODC
3
United States Agency for International Development (USAID)
3
United States Agency for International Development, Suaahara Project
3
University Teaching Hospital,
3
USAID, KNCV Tuberculosis Foundation, Challenge TB
3
Valdez Cazeneuve, R.
3
Vatican Press
3
War Child Holland
3
Water Aid
3
WHO and DOH Philippines
3
WHO Collaborating Centre on HIV and Viral Hepatitis
3
WHO Regional Office for South-East Asia
3
Wiedenmayer, K. et al.
3
World Food Programme WFP
3
World Health Organitarion
3
World Health Organization WHO, et al.
3
World Health Organization WHO, War Trauma Foundation and World Vision International
3
World Health Organization, Pan American Health Organization
3
World Health Organization, UNICEF
3
World Health Organization, Western Pacific Office
3
Xiaoyan Ke & Jing Liu
3
Штат Нью-Йорк Отдел охраны психического здоровья
3
4 Children
2
4Children
2
A. Caye
2
A. G. Lentoor
2
A. Ivanenko
2
A. Marconi
2
A. Mejia
2
A. S. Graeff-Martins
2
A. Stringaris
2
A. Tokar
2
Aagaard-Hansen, J.
2
Abdool-Gaffar, S. et al.
2
Abdulmalik, J.
2
Abela-Ridder, B.
2
ACCSI
2
Action against AIDS
2
Action Against Hunger
2
Adams, J
2
Addiss, D.
2
Advancing Partners & Communities
2
African Committee of Experts on the Rights and Welfare of the Children ACERWC
2
African Programme for Onchocerciasis Control APOC
2
AHOP
2
AIDS and Rights Alliance for Southern Africa
2
AIDSFree
2
Alliance for Public Health
2
Alzheimer's Disease International
2
Ambulatorium für Folter- und Kriegsopfer SRK
2
American Academy of Child & Adolescent Psychiatry and American Psychiatric Association
2
American Academy of Child and Adolescent Psychiatry (AACAP)
2
American Diabetes Association
2
American Society of Hospital Pharmacists (ASHP)
2
AMREF
2
and A. Rouse
2
and I. Feijo
2
and J. Rüppel
2
and S. Mauder
2
Arlington, VA: USAID’s AIDS Support and Technical Assistance Resources, AIDSTAR-One, Task Order 1
2
ASHP
2
Asian Development Bank
2
ASLM
2
Association of Indonesian Continents
2
B. Oerbeck
2
B. Vitiello
2
B. Wisner, and J. Adams
2
B.S. Kamps
2
BafF e.V.
2
Baldacchino, D.
2
Banerjee, A.
2
Beauftragte der Bundesregierung für Migration, Flüchtlinge und Integration
2
Bill & Melinda Gates Foundation
2
BMC Palliative Care
2
BMC Part of Springer Nature
2
BMC Public Health (BioMed Central)
2
Braae, U.
2
British Journal of Medicine & Medical Research
2
British Society for antimicrobial chemotherapy BSAC
2
Brot für die Welt
2
Brunner B., J. Barnes, A. Carmona et. al.
2
Bugge,J.
2
Bundesweite Arbeitsgemeinschaft der Psychosozialen Zentren für Flüchtlinge und Folteropfer – BAfF e. V
2
Burri, C.
2
C. Bachmann
2
C. C. Johnson
2
C. Ferreira-Borges
2
C. Irvine
2
C. Ködmön
2
C. M. Chern
2
C. Servili
2
CAIRN
2
Calverton, Maryland, USA: ICF International
2
Cancer Association of South Africa (CANSA)
2
Cardiovascular Diagnosis and Therapy
2
Caritas Internationalis
2
Caroline Favas
2
Catherine Moser, Conrad Frey
2
CCM Georgia
2
CDAC Network
2
Centers of Disease Control CDC
2
Central Asian Journal of Global Health
2
Central TB Divison, Ministry of Health and Social Welfare, Government of India
2
Centre d’études stratégiques de l’Afrique
2
Centre for Health & Infectious Disease Research (CHIP)
2
Centro de Coordinación de Alertas y Emergencias Sanitarias
2
Cepaz, Acion Solidaria, Convite, CodeVita, et al.
2
Charité
2
Chatanga, Peter
2
Child and Adolescent Psychiatry and Mental Health
2
Christa Hanetseder
2
CHW Central
2
CII Confederation of Indian Industry
2
Circulation
2
Circulation Research
2
ClinMed International Library
2
CMAM Forum
2
Cogliano V.J., Baan R., Straif K. et al
2
Community Eye Health Journal
2
Concern Worldwide
2
Conflict and Health
2
Congressional Research Service
2
Craig, J.
2
Cunze, S.
2
D. Daley
2
D. Haslam
2
D. M. Ndetei
2
D. Radeloff
2
D. Richardson
2
D. Walker
2
Dahal, P.
2
Damasceno, A
2
Daniel D. Moos
2
Daniel Kojo Arhinful
2
de Carvalho-Pinto, R. M.
2
Delfini Cançado, J. E.
2
Department of Health
2
Department of Health (DOH) Philippines
2
Department of Health and Human Services
2
Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ) GmbH
2
Deutsche Hauptstelle für Suchtfragen e.V.
2
Dieleman, J.L.
2
Dladla, S.
2
DNTDs
2
Dr. J. Breda
2
Dr. V. R. Kandula
2
Duke University
2
E. Abrams
2
E. Ista
2
E. Sonuga-Barke
2
E. Subata
2
E. van der Sloot
2
East, Central, and Southern African Health Community (ECSA-HC) and EngenderHealth
2
Elaine Schlosser Lewis Fund
2
Elmqvist, T.
2
Elsevier Ltd.
2
EMHJ – Vol. 30 No. 12 – 2024
2
Engender Health Society (Improving Women's Health Worldwide)
2
ERS
2
Escuela de Salud Publica
2
ESMO
2
Ethiopian Health and Nutrition Research Institute
2
Ethno-Medizinisches Zentrum e.V.
2
EU
2
Eurasian Harm Reduction Network
2
European Interagency Security Forum (EISF)
2
European Scientific Journal
2
F. Nakagawa
2
F. Pérez
2
F. Saini
2
F. Stuer
2
FAO, IFAD, UNICEF, WFP and WHO
2
Federal Ministry of Health, Dept. of Public Health, National HIV
2
Federal Ministry of Health, Federal Republic of Nigeria
2
Federal Ministry of Health, Uganda
2
Fegert, J.M.
2
FG Consulting Group, C. Daniels, C. Smyth et al.
2
First Draft, Yale Insitute for Global Health
2
Fistula Care
2
Fleischer, K. et al.
2
Fondo de Poblaciones de las Naciones Unidas - UNFPA
2
Food and Agriculture Organization (FAO)
2
Food, Medicine and Health care Administration and Control Authority of Ethiopia (FMHACA)
2
Frontiers in Cardiovascular Medicine
2
Frontiers in Pediatrics
2
G. Harper
2
G. K. Siberry
2
G. Ravasi
2
G. Venugopal
2
G. Walter
2
G. Williams, E. Alarcón, S. Jittimanee et al.
2
Garcia, P.J.
2
Germanwatch
2
Gesellschaft für Thrombose-undHämostaseforschung e.V. GTH
2
Ghana Health Service
2
Global Financing Facility (GFF)
2
Global Fund
2
Global Handwashing Partnership
2
Global Initiative for Asthma
2
Globalization and Health
2
Gobierno Bolivariano de Venezuela, et al.
2
Governement of Nepal, Ministry of Health
2
Governement of Nepal, Ministry of Health and Population, Department of Health Services
2
Government of Kenya
2
Government of Malawi
2
Government of Nepal Ministry of Health and Population Family Health Division
2
Government of Sierra Leone, Ministry of Health and Sanitation
2
Government of Tanzania
2
Government of the People's Republic of Bangladesh DGHS Directorate General of Health Services Ministry of Health and Family Welfare
2
Government of the Republic of Mozambique
2
Graves C.
2
Gregory, J.
2
H. Gosney
2
H. Ingold
2
H. Knoester
2
H. Kristensen
2
H. Metzger
2
H. Zainiddinov
2
H.L. Nguyen
2
H6 Partnership
2
Handicap International
2
Health Care Without Harm
2
Health Policy Plus
2
Health System Trust
2
HEART
2
HelpAge International, et al.
2
Hesperian Foundation
2
Hesperian Health Guides
2
Hoffmann, C.
2
Horton, Susan, et al.
2
Husain, M.J.
2
IASC
2
ICAP Columbia University (Mailman School of Public Health)
2
ICF Macro
2
ICRC and International Federation of Red Cross and Red Crescent Societies
2
IDS
2
IFRC - International Federation of Red Cross
2
Indian Nursing Council
2
Institute for Health Metrics and Evaluation (IHME)
2
Institutional Repository for Information Sharing iris
2
Inter-Agency Network for Education in Emergencies
2
Inter-agency Task Force on Financing for Development
2
International Alert, Global Initiative on Psychiatry
2
International Bank for Reconstruction and Development/ The World Bank
2
International Bureau for Epilepsy
2
International Coalition for Trachoma Control ICTC
2
International commitee of the Red Cross
2
International Committee of the Red Cross
2
International Committee of the Red Cross ICRC
2
International Diabetes Federation
2
International Federation of Red Cross and Red Crescent Societies (IFRC)
2
International Journal for Equity in Health
2
International Journal of Health Policy and Management IJHPM
2
International Labour Organization
2
International League Against Epilepsy
2
International Medical Corps
2
International Society for infectious Diseases
2
IntraHealth International
2
IPAS
2
IPCC
2
IPPF
2
J. - P. Raynaud
2
J. Ananworanich
2
j. Bushati
2
J. D. Machado
2
J. Hourcade Bellocq
2
J. J. Hudziak
2
J. Keatley
2
J. L. Turban
2
J. M. Nagata
2
J. N. M. Schieveld
2
J. Pei-Chen Chang
2
J. V. Lazarus
2
Johns Hopkins Bloomberg School of Public Health , Syrian American Medical Society, et al.
2
Joseph M Rey
2
Journal of Clinical Medicine
2
Journal of Public Health
2
Journal of the American College of Cardiology
2
Journal of the International Association of Providers of AIDS Care
2
Journal of Virus Eradication
2
Juniper, E. F.
2
juris GmbH
2
K. Greenaway
2
K. Manassis
2
K. O’Loughlin
2
K. Quy
2
K. R. Overgaard
2
Kann, S.
2
Khaltaev, N.
2
Kohler, S.
2
Kola, L.
2
Kompetenznetz Public Health zu COVID-19
2
Kompetenznetz Pulic Health Covid-19
2
L. A. Rohde
2
L. Barrera
2
L. Newman
2
L. Pacione
2
L. Sereno
2
Lesley Odendal
2
London School of Hygiene & Tropical Medicine, et al.
2
Lu, C.
2
Lungenliga Schweiz, Bundesamt für Gesundheit
2
M. Archary
2
M. Bakare
2
M. Cabra
2
M. Conceição do Rosário
2
M. Dara
2
M. Doherty
2
M. Ferrin
2
M. Holtmann
2
M. Mansfeld
2
M. Penazzato
2
M. R. Sanders
2
M. Ristola
2
M. Snowling
2
M. Vicari
2
M. Vitoria
2
Maitland, K.
2
MamaYe Sierra Leone
2
Mamel Quelapio, Maria Idrissova, Gunta Dravniece et al.
2
MapAction
2
Marais, J.F.
2
Martinez-Alvarez, M.
2
Mary Amuyunzu-Nyamongo
2
Maternal & Childhealth Advocacy International MCAI
2
Mazigo, H.
2
McGahey, Christopher
2
MCHIP
2
MEASURE
2
Medécins sans Frontières MSF
2
Medical Peace Work
2
Medical Society Consortium on Climate and Health
2
Menezes Pizzichini, M. M.
2
Mensah, G.A.
2
Mental Health America
2
Mental Health First Aid
2
Médecins du Monde
2
Ministerio da Saude Brasil
2
Ministerio da Saude, Brazil
2
Ministerio da Saude, CONASS, Conasems et al.
2
Ministerio de Salud - Chile
2
Ministerio de Salud - Peru
2
Ministerio de salud pública y bienestar social, Paraguay
2
Ministerio de salud y deportes, Bolivia
2
Ministerio de Salud y Protección Social
2
Ministerio de Salud y Protección Social, Colombia
2
Ministerio de Salud, Bolivia
2
Ministerio der Salud Argentina
2
Ministère de la Santé
2
Ministère de la Santé Senegal
2
Ministère de la Santé, Burkina Faso
2
Ministère de la Santé, République du Bénin
2
Ministério da Saúde de Moçambique
2
Ministério da Saúde, Brazil
2
Ministry of Health & Family Welfare Government of India
2
Ministry of Health and Family Welfare Government of the People's Republic of Bangladesh
2
Ministry of Health and Population, Nepal
2
Ministry of Health and Social Welfare Liberia
2
Ministry of Health& Family Welfare, Goverment of India
2
Ministry of Health, Federal Democratic Republic of Ethiopia
2
Ministry of Health, Kingdom of Lesotho
2
Ministry of Health, Republic of South Africa
2
Ministry of Health, Tanzania
2
Misereor, Brot für die Welt, Global Policy Forum GPF
2
Mission Rabies
2
Mortimer, K.
2
Mphahlele, R.E. et al.
2
MSH
2
Mugomeri, Eltony
2
Murray, C.J.L.
2
N. Ait-Khaled, D. Enarson
2
N. Ford
2
N. Habibov
2
Naidoo, K.L.
2
National Academies of Sciences, Engineering, and Medicine
2
National Agency for Food and Drugs Administration and Control (NAFDAC)
2
National AIDS Control Council
2
National AIDS Control Programme (NACP) & Reproductive and Child Health Section
2
National Centre for AIDS and STD Control (NCASC)
2
National Coordination Committee, Jan Swasthya Sabha
2
National Council on Disability Affairs (NCDA)
2
National Health Education Information and Communication Centre, Ministry of Health and Population, Governement of Nepal
2
National Health Insurance Scheme
2
National Institute for Health and Care Excellence (NICE)
2
National Institute on Drug Abuse
2
National Leprosy Eradication Programme
2
NCD Alliance
2
Ndlovu, V.
2
Nepal Red Cross Society
2
Neurology Asia
2
New England Journal of Medicine
2
Norwegian Refugee Council, Internal Displacement Monitoring Centre
2
NSW Health and University of Western Sydney
2
O. Chokoshvili
2
Observatoire européen des drogues et des toxicomanies
2
Observatorio Europeo de las Drogas y las Toxicomanías
2
Ol. Kazakova, D. Krupchanka, et al.
2
Open Journal of Epidemiology
2
Organisation for Economic Co-operation and Development (OECD)
2
Organisation Mondiale de la Santé OMS, et al.
2
Organisation panaméricaine de la Santé
2
Organización Mundial de la Salud (Americas)
2
Organización Mundial de la Salud (OMS)
2
Oxford University Press
2
P. Clayden
2
P. Hay
2
P. J. Frick
2
PACK
2
PAHO Pan American Health Organization, Enfant du Monde
2
PAHO, ICW-LATINA
2
Pan American Health Organisation (PAHO)
2
PATA
2
Pitt, C.
2
PLOS Neclected Tropical Diseases
2
PLOS Medecine
2
PMC (US National Library of Medicine National Institutes of Health)
2
PMC (US National Library of Medicine National Institutes of Health)
2
Population Foundation of India
2
Prince, M., and J. Jackson
2
Programme national de lutte contre le paludisme - Sénégal
2
Public Health Institute
2
Puchalski, C.M.
2
Pusat Penanggulangan Krisis Kesehatan
2
Q.M. Trinh
2
R. C. Vreeman
2
R. Granich
2
R. Humeniuk, S. Henry-Edwards, R. Ali
2
R. Lovich
2
R. S. Mastrorosa
2
R. Vermeiren
2
Reddel, H. K.
2
Refugees International
2
Regional Network for Equity in Health in east and southern Africa (EQUINET)
2
Republic of South Africa
2
Revista Panamericana de Salud Pública
2
RKI
2
Robert Koch Institut (RKI)
2
RüppelT.
2
S. Cortese
2
S. Gwavuya
2
S. MacPhee
2
S. Nag
2
S. Scott
2
S. Seedat
2
S. Shadianloo
2
S. W. Henderson
2
S. Wanderer
2
SAGE Journals
2
Sallam, M.
2
Samwel Mbugua, Kerry L. D. MacQuarrie
2
Sangath
2
Sarah Frost, Kylie Mines, Jamie Noon, Elsje Scheffler, and Rebecca Jackson Stoeckle
2
Schäferhoff, M.
2
Schneider M. et al.
2
Scientific Electronic Library Online
2
Scientific Research Publishing
2
SCMS
2
Secretaria de Atenção à Saúde Departamento de Ações Programáticas Estratégicas
2
Secretaria de Estado de Saúde de Minas Gerais (SES-MG)
2
Secretaria de Estado de Saúde de Minas Gerais (SES-MG), Brasil
2
Secretaría de la Función Pública, Paraguay
2
Secretaría de Salud de México
2
See text
2
Seitz, K.
2
Sibanda, E.
2
Smithsonian Science Education Center
2
Smithsonian Science Education Center, et al.
2
Sociedad Venezolana de Salud Pública
2
Sociedad Venezolana de Salud Pública Red Defendamos la Epidemiología Nacional
2
South African Family Practice
2
Southern African HIV Clinicians Society
2
Springer
2
Starling
2
STRIVE
2
Sunil Daryanani
2
T. Colton
2
T. D. Benton
2
T. M. Achenbach
2
T. Measham
2
T. Noori
2
T. Poteat
2
T. Tsertsvadze
2
T. Z. Ting Fang
2
T.Samudio, P.Ovelar, et al.
2
Tarun Dua, Nicolas Clark, Neerja Chowdhary et al.
2
TB Alliance
2
Terre des Hommes
2
The Brazilian Journal of Infectious Diseases
2
The Ethiopian Public Health Institute, Federal Ministry of Health Ethiopia
2
The Federal Democratic Republic of Ethiopia
2
The International Union Against Tuberculosis and Lung Disease
2
The Lancet healthy Longevity
2
The Lancet, Planetary Health
2
The Public Good Projects
2
The Republic of the Union of Myanmar, Ministry of Environmental Conservation and Forestry
2
The Republic of the Union of Myanmar, Ministry of Natural Resources and Environmental Conservation
2
The Sanitation Learning Hub
2
The South African Medical Journal
2
Theo Smart
2
Translation without Borders
2
U.S. President's Malaria Initiative (PMI), CDC, USAID, et al.
2
UCL
2
Umbas, R., S. Hardjowijoto, C.A. Mochtar, et al.,
2
UN
2
UN Children's Fund
2
UN Environment
2
UN Environment Programme
2
UN High Commissioner for Refugees
2
UN Office for the Coordination of Humanitarian Affairs, UN Country Team in Yemen
2
UNAIDS (Joint United Nations Programme on HIV
2
UNAIDS (Joint United Nations Programme on HIV
2
UNAIDS, UNODC (United Nations Office on Drugs and Crime)
2
UNEP
2
UNESCO's International Programme for the Development of Communication (IPDC)
2
UNFPA, Save the Children USA
2
UNICEF and GOARN
2
UNICEF Indonesia
2
UNICEF, WHO
2
UNICEF, World Health Organization WHO
2
Union Internationale Contre la Tuberculose et les Maladies Respiratoires
2
Unitaid (Innovation in Global Health)
2
United Nations (UN)
2
United Nations Development Programme
2
United Nations Office on Drugs and Crime UNODC
2
United Nations Population Fund UNFPA
2
United States of America - Department of State
2
Universidad Católica Andrés Bello
2
University of Malawi
2
UNODC (United Nations Office on Drugs and Crime)
2
UNOPS, Stop TB Partnership et al.
2
US Dept. of Health and Human Services
2
USAID Deliver Project
2
USAID From the American People
2
USAID, Health Systems 20
2
USAID, SIAPS
2
USAID, SPRING
2
V. Allread
2
V. Patel
2
V. Roessner
2
Van de Sande, W.
2
van Herwijnen, T., Ritchie, S. & Eaton, J.
2
Velisha Ann Perumal-Pillay & Fatima Suleman
2
Washington Group on Disability Statistics
2
Water, Engineering and Development Centre (WEDC) Loughborough University, UK
2
WaterAid
2
Watts, S.
2
Welthungerhilfe e.V.
2
WHO Europe
2
WHO Regional Office for Europe
2
WHO Universal Health Coverage
2
WHO, UNICEF
2
World
2
World Alliance for Patient Safety
2
World Business Council for Sustainable Development (WBCSD)
2
World Drug Report 2017
2
World Health Organization (WHO), Regional Office of the Western Pacific
2
World Health Organization (WHO), International Water Association (IWA)
2
World Health Organization (WHO), National Center on Birth Defects and Developmental Disabilities from the United States Centers for Disease Control and Prevention (CDC), International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR)
2
World Health Organization (WHO), Regional Office for the Western Pacific
2
World Health Organization WHO, Bangladesh
2
World Health Organization WHO, IFRC
2
World Health Organization WHO, Regional Office for Africa
2
World Health Organization WHO, Western Pacific Region
2
World Health Organization, Stop TB Partnership
2
World Health Organization, Regional Office for South-East Asia
2
World Health Organization, Regional Office for the Western Pacific
2
World Health Organization. Regional Office for Europe
2
X. Chen
2
Y. Ono
2
Yamey G.
2
Zambia Medicines Regulatory Authority (ZAMRA)
2
Всемирная Организация Здравоохранения - Европейское региональное бюро
2
Всемирная организация здравоохранения (Eвропейское)
2
Департамент здравоохранения города Москвы
2
Саратовский научно-медицинский журнал.
2
(CDC) Center for disease control and prevention
1
(World Psychiatry
1
, M. K. C. Nair
1
, S. Evans‐Lacko
1
, S. Eymard-Duvernay
1
. Amini
1
1000 Cities 1000 Lives
1
2011
1
2012
1
2016
1
2018
1
390: 898&ndash
1
3ie Impact
1
4 Children (Coordinating Comprehensive Care for Children)
1
912
1
[Asian Disaster Preparedness Center (ADPC)]
1
A, Figueroa
1
A.
1
A. Rimoin
1
A. A. Neilson, C. A. Mayer
1
A. A. Olashore
1
A. Abdul-Quader
1
A. Abdul-Quader, M. Berry, T. Bingham
1
A. Abdulmoneim
1
A. Adesina
1
A. Alebel
1
A. Alexandrova
1
A. Amouzou
1
A. Anand, J. Sandefur, and A. Subramanian
1
A. Arzimanoglou
1
A. August Burns, Ronnie Lovich, Jane Maxwell, Katharine Shapiro
1
A. Ball
1
A. Baller, et al.
1
A. Baumann, C. Hofstetter, et al.
1
A. Bello Cherifath
1
A. Benson
1
A. Benzacar
1
A. Benzaken
1
A. Bokazhanova
1
A. Boltaev
1
A. Brotherton
1
A. Brown
1
A. C. Hesseling, M. F. Cotton, C. F. von Reyn, et al.
1
A. Caye, P. J Frick & L. A Rohde
1
A. Chiumento
1
A. Chu, Z. Li et al.
1
A. Cohen, J. Eaton, B. Radtke, et al.
1
A. Colson
1
A. Cournil
1
A. D. Meundi, M. D. Meundi, B. B. Dhabadi
1
A. D. Meundi, M. D. Meundi, B. B. Dhabadi, et al.
1
A. Delpak, et al.
1
A. dos Santos Filho, W. Marques, P. Dourado, et al.
1
A. E. Kendall
1
A. E. Miranda
1
A. Figueroa
1
A. Fouda Bita et. al.
1
A. Freitez, M. González and G. Zúñiga
1
A. Fuchs
1
A. García-Prado, J.P. Sarmiento, et al.
1
A. Gebrie
1
A. Gheorghe
1
A. Goba, et al.
1
A. Goga
1
A. Grimsrud
1
A. Gupta
1
A. H. Sohn
1
A. Haakenstad et al.
1
A. Haenen
1
A. Hanciles-Amu
1
A. Harxhi
1
A. Harxkhi, et al.
1
A. Horban
1
A. Imohe, J. Krasevec et al.
1
A. Isehak
1
A. IYANE SOW
1
A. J. Flisher
1
A. J. Gage
1
A. J. M. Cho
1
A. J. Prendergas
1
A. J. Shattock
1
A. Jain
1
A. Jindani, A. Nunn, D. A. Enarson
1
A. Judd
1
A. K. Lam
1
A. Kanabus
1
A. Kanchar
1
A. Kapilashrami
1
A. Karimi, R. M. Ghanaie
1
A. L. Drake
1
A. L. P. Batista
1
A. L. Slogrove
1
A. L. Wirtz
1
A. L.C. de Vries, K. J. Zucker
1
A. Lachman
1
A. Landry, et al.
1
A. LC de Vries
1
A. Liland
1
A. Locke, N. Kirst, C.G. Shultz
1
A. Long
1
A. Lwidiko
1
A. Lycett
1
A. M. Loeffler, F. J. Curry
1
A. M. Rosasco
1
A. M. Tavares
1
A. Mahieu
1
A. Malaza
1
A. Malik, M.Li, et al.
1
A. Medhanyie, M. Spigt, Y. Kifle, et al.
1
A. Menon
1
A. Mijch
1
A. Minter, J. Edmunds et al.
1
A. Miruka
1
A. Moniruzzaman
1
A. Moolla, S. Kgowedi et al.
1
A. Muñoz del Carpio Toia
1
A. Murray-Zmijewski
1
A. Mwangi
1
A. Nasheeda
1
A. Naveed, K. Wing, et al
1
A. Nicholson
1
A. Ntamwishimiro Soumare, et B. my Semegan
1
A. Nunes Gonzalez, et al.
1
A. Nyundo
1
A. O. Rojas Vistorte , W. Ribeiro, C. Ziebold, et al.
1
A. Ojoo, B. Amugune et al.
1
A. P. C. F. Freire
1
A. Pawlowski, M. Jansson, M. Sköld, et al.
1
A. Pereira, B. do Valle Pinheiro et al.
1
A. Pharris
1
A. Phillips
1
A. Pirani
1
A. Prüss-Ustün
1
A. Rakotoarisoa, L. Randrianasolo, S. Tempia, et al.
1
A. Rihan
1
A. Ronan
1
A. Roy, M. Eisenhut, R. . Harris, et al.
1
A. Russolillo
1
A. Silveira
1
A. Sondheimer
1
A. Sriram
1
A. Stavropoulou, A. Philalidis, et al.
1
A. Stein
1
A. Stengaard
1
A. T. Choko
1
A. T. Makadzange
1
A. Tami, M.E. Grillet, et al.
1
A. Tausch
1
A. Teltschik
1
A. Terlikbayeva, S. Hermosilla, S. Galea, et al.
1
A. Tursynbayeva
1
A. van Ahee
1
A. Vieno
1
A. Volokha
1
A. W. Gold
1
A. Warnke
1
A. Welbourn
1
A. Wirtz
1
A. Xhuvani
1
A. Yager
1
A. Zumla
1
A.-C. ZK Bissek
1
A.B. A. Boxall, D. W. Kolpin, et al.
1
A.C. Barbosa Caetano, J.C. Wenceslau Cocovich et al.
1
A.C. Ubesie
1
A.D. Négrel, H.R. Taylor and S. West
1
A.Goncé, A. Hawkins-Villarreal et al.
1
A.L: Fanning
1
A.Lachman
1
A.Mavrodaris
1
A.Naess Herstad
1
A.O. Dieng, I. Diallo et. al.
1
A.R. Orihuela
1
A.Ramesh
1
A.Sullivan
1
A.W. Gelb, W.W. Morriss, W. Johnson, et al.
1
Aantjes, C.
1
Aaron M Kipp, Margaret Maimbolwa, Marie A Brault et al.
1
Aarthi, G.R.
1
Abbara, A.
1
Abdala, M et al
1
Abdel-All, M
1
Abdoulaye F., M. Bop, A. Kane
1
Abdul Rahim, H.F.
1
Abdulkareem, B.
1
Abdulrahim, D.
1
Abebaw Fekadu, Girmay Medhin, Medhin Selamu, et al.
1
Abebe, B.
1
Abeje Fekadu, G. F. Ambaw Getahun
1
Abela-Ridder, B. et al.
1
Abera, M.
1
Abetz, L.
1
Abhaskhanian, A.
1
Abida Haq binti Syed M. Haq et al.
1
Abir, T.
1
Ablo Prudence Wachinou, Serge Ade, Gildas Agodokpessi, Berenice Awanou, Dissou Affolabi, Wilfried Bekou, Marius Esse, Gabriel Ade, Severin Anagonou, Anthony D. Harries,1Programme National contre la Tuberculose (PNT), Cotonou, Bénin
1
Abola, M. T. B.
1
Aboud S., R. Mdegela
1
Abras A., Ballart C., Fernández-Arévalo A., et al.
1
Abu Mouch et al.
1
Abubakar, A.
1
Abubakar, B.K.
1
Abuga, J.A.
1
Academia Nacional de Medicina (ANM)
1
Academic Journal of Interdisciplinary Studies MCSER Publishing
1
Academic Journals
1
Academicus (International Scientific Journal)
1
ACAPS
1
ACC
1
Access Campaign, Médecins sans Frontières
1
Access Living
1
Access to Medicine Foundation
1
ACCSI, CIAT
1
ACCSI, ICASO
1
Aceite o Desafio (Terminemos com a AIDS)
1
ACF International
1
ACF International Network
1
ACF International Network and the Oakland Institute
1
ACF International, SIDA
1
Achary A.
1
Acharya, S., S. Sharma, B. Dulal, K. Aryal
1
Achoki, T., M. K. Miller-Petrie, S.D. Glenn, et al.
1
Acibadem University, Atasehir-Istanbul, Turkey
1
ACIN
1
ACPF, Plan International
1
ACT Watch Group et al
1
Acta Scientific Medical Sciences
1
ACTafrica, HNP
1
Action Aid
1
Action Contre la Faim (ACF) International,
1
Action contre la Faim France
1
ACTION global health advocacy partnership
1
Action on Anitbiotic Resistance (ReAct)
1
ACTION partner oranizations
1
Adachi, Y.
1
Adam C. Levine, M.D., M.P.H., Pranav P. Shetty, M.D., M.P.H., Patricia C. Henwood, M.D., Pardis Sabeti, M.D., Joel T. Katz, M.D., and Anand Vaidya, M.D.
1
Adams, J.
1
Aday A.W.
1
ADCAP Age & Disability Capacity
1
Addo-Yobo, E. et al.
1
Adebowale T., Umukoro O., Gater R., et al.
1
Adela Cayetano, R.D.
1
Adelekan, B.
1
adelphi
1
Adhikari, B.
1
Adler, A.J.
1
Adolescent Division, Ministry of Health and Social Welfare, Government of India
1
Adrian Angold & Elizabeth J. Costello
1
Adrian Sondheimer
1
Adrian Sondheimer, Joseph M Rey, Переводчик: Константин Мужановский
1
Adriana Jiménez Rojas
1
Advantage Africa, FIRAH, Resource Center Applied Research and Disability
1
AECT
1
AfClix
1
AFEW
1
Africa CDC Centers for Disease Control and Prevention
1
Africa Region
1
African Centre for the Constructive Resolution of Disputes
1
African Centre for Treatment and Rehabilitation of Torture Victims (ACTV)
1
African Development Bank
1
African Disability Rights Yearbook
1
African Evaluation Journal
1
African Field Epidemiology Network (AFENET)
1
African Journal of Laboratory Medicine
1
African Journal of Pharmacy and Pharmacology
1
African Journal of Primary Health Care & Family Medicine
1
African Journal of Primary Health Care & Family Medicine (PHCFM)
1
African Journal of Primary Health Care & Family Medicine, AOSIS
1
African Journal of Thoracic and Critical Care Medicine
1
African Journals Online (AJOL)
1
African Population and Health Research Centre APHRC
1
African Population Studies
1
African Prgramme for Onchocerciasis Control
1
African Religious Health Assets Programme (ARHAP)
1
African Union of the Blind (AFUB), Cameroon National Association for the Blind (CNAB)
1
African Union, Africa CDC
1
African Union, African CDC, World Health Organisation
1
AfrOx
1
Afshin, A.
1
Aftab Ala, Elizabeth Boxall, Steven Bradley et al.
1
Afulani PA, Nutor JJ, Agbadi P, Gyamerah AO, Musana J, Aborigo RA, et al.
1
Agar Brugiavini and Noemi Pace
1
Agarwal, A.
1
Agbiji E., Agbiji O.M.
1
Agbor, V.N.
1
AGEF
1
Agence de plannification et de coordination du NEPAD
1
Agence national de la statistique et de la Démographie (ANSD)
1
Agencia Espanola de Cooperación International para el Desarrollo
1
Agencia Espanola de Cooperatión International para el Desarrollo
1
Agentur der Europäischen Union für Grundrechte
1
Ager, D., Oele, G., Muhula, S., et al
1
Agne Diminskyte
1
Agoons, B.B.
1
Agora Research Letter
1
Agriculture for Impact-Imperial College of London
1
Aguayo, Victor M. et al.
1
Agudelo Calderón,C.
1
Agudo C. T., Nattez S.G.V.
1
Aguilar-León, P et al.
1
Agyepong I. et al.
1
Ahanhanzo, Y.
1
Ahmad, U., Chau, D.M. et al.
1
Ahmed Mohamed Abdel Shafi and Reem Mohamed Abdel Shafi
1
AHOP National Centre based in Nigeria
1
Ahumada A., Ebensperger R. et al
1
Ahumada, K.
1
AI.COMM
1
AIDS
1
AIDS & TB Programme
1
AIDS Care Psychological and Socio-medical Aspects of AIDS/HIV
1
AIDS Education Training Center AETC
1
Aids Fonds, KELIN
1
AIDS Foundation (Until no child has AIDS)
1
AIDS Free (Strenghtening High Impact Interventions for a AIDS-free Generation)
1
AIDS Research and Therapy
1
AIDS Support and Technical Assistance Resources Project,
1
Aidsfonds
1
Aidsmap
1
Aidstar-One
1
AIEPI Hospitalario
1
AIIPC
1
Aiken L., Simonetti M., Sloane D., et al.
1
AIWG
1
Ajijola, O.A. et al.
1
Ajit Pradhan, Pradeep Poudel, Deborah Thomas, Sarah Barnett
1
akkon Hochschule für Humanwissenschaften
1
Akpenpuun Joyce Rumun
1
Aksion Plus
1
Aksoy, S.
1
Aktionbündnis gegen AIDS
1
Aktionsbündnis gegen AIDS
1
Al Delaimy W., Ramanathan V., Sanchez Sorondo M. et al.
1
Al Himaya Foundation for Trauma Recovery, Growth and Resilience
1
Al Moosawi, S.
1
Al-Maaitah, R., Conlan, L., Gebbie, K. et al.
1
Al-Shorbaji, Najeeb, Atun, Rifat, Car, Josip, Majeed, Azeem, Wheeler, Erica.
1
Alak, ACD.
1
Alam K., Shah A.K., Ojah P., et al.
1
Alan J Budney & Catherine Stanger
1
Alan J Flisher
1
Alarcón, V.
1
Alarcón-Yaquetto
1
Albania Center for Population and Development (ACPD)
1
Albanian Association of People Living with HIV/AIS
1
Alberto Minoletti, Michelle Funk, Natalie Drew et al.
1
Albrechtsen N., Torekov S., Holst J.
1
Alcáron de Noya, B.
1
Aleksandrowicz L., Green R., Joy E., et al.
1
Alemayehu Tibebe and Kenfe Tesfay
1
Alexander Lourdes Samy, Zahra Fazli Khalaf, & Wah-Yun Low
1
Alexander von Gontard
1
Alexianer St. Hedwig-Krankenhaus
1
Alice Mark
1
Alice Payne Merritt, Gabrielle Hunter, Anne Ballard et al.
1
Aliga C., Mutyabule J., Nakate G., et al.
1
Aliku, T. et al.
1
Alimardani, M. and Mona Elswah
1
Alimonte, Mary D'
1
Alipanah N, Jarlsberg L et al.
1
Aljadeeah, S.
1
Allach, Y.
1
Allers, Claudia, Timothy O’Hearn, and Meba Kagone
1
Alliance for Health Policy and Systems Research
1
Alliance of Bioversity & CIAT
1
Allied Publishers Private LTD.
1
Alliot C.
1
Allwood, B.
1
Almeida C
1
Almudena Marí Saéz, Sabrina Weiss, Kathrin Nowak,et al.
1
ALNAP, Provention Consortium
1
ALNAP-CDA
1
Alonso González, Mónica
1
Alonso, J.
1
Alonso-Sardón, M.
1
Altcheh, J.
1
Alva Träbert
1
Alva-Díaz, C.
1
Alvarado R., Ramírez J. et al
1
Alves Dias, C.
1
Alves J.D., Abade A.S., Peres W.P. et al.
1
Alys, W.
1
Alyssa S. Parpia, Martial L. Ndeffo-Mbah, Natasha S. Wenzel, et al.
1
Alzheimer's Association
1
Amalia Panzarelli
1
Amanda Mattsson
1
Amaya M Gillespie, Rafael Obregon, Rania El Asawi, et al.
1
Amber Hsiao
1
AmC
1
American Academy of Child and Adolescent Psychiatry
1
American Academy of Family Physicians
1
American Academy of Paediatrics
1
American Academy of Pediatrics
1
American College of Chest Physicians
1
American Heart Association
1
American Journal of Obstetrics and Gynecology
1
American Journal of Physiology - Lung Cellular and Molecular Physiology
1
American Journal of Psychiatry
1
American Nurses Association
1
American Psychiatric Association
1
American Public Health Association
1
American Research Foundation,
1
American Thoracic Society
1
AmfAR
1
Amina Mushtaq, Attiya Inam, Muhammad Abiodullah
1
Amini, M.
1
Amnesty International
1
Amodeo, C. et al.
1
AMR Industry Alliance
1
AMSHeR (American Men for sexual Health & Rights)
1
Amterdam Institute for Global health & Development aighd
1
Amy Bloom, Leo Blanc, Chris Dye et al.
1
Ana Beatriz Monteiro Costa, Mario Gyoeri and Fábio Veras Soares
1
Ana Carvajal, Amando Martín, Enrique Blanco, et al.
1
Ana Carvajal, José Félix Oletta López, Alejandro Rísquez
1
Ana Cecília Gomes Rosa Luiz, Bruna Silveira Caixeta, Milena Ferreira Cruvinel et al.
1
Ana Figueroa, Cesar Soutullo, Yoshiro Ono & Kazuhiko Saito
1
Ana Flor Hexel Cornely, João Gabriel Flôres da Rocha
1
Ana Maria Henao-Restrepo, Ira M Longini, Matthias Egger, et al.
1
Anahi Ayala Iacucci, R. Copeland, Z. Mamood, et al.
1
Anand, S.
1
Anand, Shuchi
1
Anaya-Covarrubias, J.Y.
1
Anayda Portela, Helen Smith, Cicely Marston
1
and J. Latimer
1
and A. Kent
1
and A. Trojan
1
and A.M.Chirinos-Leañez
1
and B.M. Ances
1
and C. Agbedia
1
and C. Sabine
1
and C. Wonodi
1
and C. Zimmer
1
and C.J. Arnson
1
and C.L.Weeraratne
1
and D. Samarashinghe
1
and D.V.Havlir
1
and E. Möhler
1
and G. Breed
1
and I. Walker
1
and I.Falkenberg
1
and J. Elkins
1
and J. Garcia-Rosales Delgado
1
and J. M. Cohen
1
and J. Roberto
1
and K. S. Jacob
1
and K.R. Smith
1
and L. Reilly
1
and L.M.Morel
1
and M.S. Walker
1
and O. Bowden-Jones
1
and P. A M Schreuder
1
and P. Heydt
1
and Papadakis Maxine
1
and S. Ayenalam Kidanie
1
and S. Fung Lee
1
and S.J. Mason
1
and T. Clasen
1
and T. Rüppel
1
and W. Scholten
1
Anderson, H.R.
1
Anderson, L.
1
Andersson E., Frantzeskaki N., et al.
1
Andrade, D.
1
Andreas Sandgren, Marieke J. van der Werf, Netta Beer et al.
1
Andrew Garnett, Ticky Raubenheimer, Debra Kristensen et al.
1
Andrew S Azman, Lucy A Parker, John Rumunu, et al.
1
André Biakowski, Martin Halotta, Thilo Schöne,
1
André Yébakima
1
Andrianos, L.
1
Angela Schuster, Christoph Heintze
1
Angelo Barbato, Martine Vallarino, Filippo Rapisarda, et al.
1
Angheben, A. et al.
1
Angwenyi, V.
1
Ann Ashworth et al.
1
Ann Indian Acad Neurol
1
Anna Melissa S. Guerrero
1
Annah Wamae, George Kichamu, Francis Kundu, Irene Muhunzu
1
Annals of General Psychiatry
1
Anne Beugny, Pr Olivier Bouchaud, Dr. Charles Kouanfack et. al.
1
Anne Niedermeier
1
Annelies Heijmans
1
Annim, Samuel Kobina, Kofi Awusabo-Asare, and Joshua Amo-Adjei
1
Annual Reviews
1
Ansumana, R.
1
Antares foundation
1
Anthonisen, N.R.
1
Antimicrobial Resistance & Infection Control
1
Antonia Braus, Maria Victoria Larrateguy, Angela R. Schug, Johan Willems
1
Antonia Braus, Maria Victoria Larrateguy , Angela R. Schug, Johan Willems
1
Anushka Kalyanpur
1
ANVISA Agência Nacional de Vigilância Sanitária
1
Anxiety Canada
1
AOSIS Publishing
1
Aparecida Vincent, V. et al.
1
APB
1
Apisarnthanarak A.,S. Danchaivijitr,T. Khawcharoenporn, et al.
1
APMG Health
1
Aporia
1
Appleton, R.E. & Cross, J.H.
1
Appuhamy, R.
1
Aquaclara, et al.
1
Ar-Rizqi, M.A.
1
Arakaki-Sanchez
1
Aranka Anema1,2*, C. G. Au-Yeung
1
Arantes Beatriz, L. B.
1
Arbeitskreises Blut des Bundesministeriums für Gesundheit
1
Arbo, A.
1
Arch Argent Pediatr
1
Ardath Grills, Stephanie Morrison, Bradley Nelson et al.
1
Arens-Azevêdo U.
1
Argote P., Barhan E., Zukerman Daly S. et al.
1
Arii M., F. Baele, J. Bedford et al.
1
Arima Mishra
1
Aristizabal, A.
1
Arjadi , R.
1
Arlington, VA: Management Sciences for Health
1
Armed Forces Pest Management Board, USA
1
Armenian National AIDS Center
1
Armocida, B.
1
Armstrong, G.
1
Armstrong, J.
1
Arne H Eide and Yusman Kamaleri
1
Aron, M.B. et al.
1
Arq Neuropsiquiatr
1
Arquivos Brasileiros de Cardiologia
1
Arregoces L. et al.
1
Arrieta, A.
1
Ars edition
1
ARTE
1
Asa, S.S., A. Titilayo, and J. A. Kupoluyi.
1
Asaduzzaman, M. et al.
1
Asakura S.
1
ASEDP (Asociación Salvadoreña para el Estudio y Tratamiento del Dolor y Cuidados Paliativos)
1
Ashby B.
1
Ashdin Publishing Journal of Drig and Alcohol Research
1
Asher, M.I.
1
Ashish KC, R. Gurung, M.V Kinney, et al.
1
Ashish, K.C.
1
Ashleigh Tuite
1
ashm hiv management in Austalasia
1
Ashworth, Ann et al.
1
Asian American Psychological Leadership (AAPA)
1
Asian-Pacific Resource & Research C0entre for Women (ARROW)
1
Asociación Colombiana de Neumología Pediátrica
1
Assaf S., W. Wang, L. Mallick
1
Assaf, Shireen and Rebecca Winter
1
Assaf, Shireen, Sarah Staveteig, and Francine Birungi
1
Assegaai, T. and H. Schneider
1
Assemblée Nationale, République du Benin
1
Association française des anthropologues
1
Astle. B.
1
Atal Bihari Vajpayee Institute of Good Governance & Policy Analysis
1
Aten, J.
1
Ateudjieu, J.
1
Atlantes
1
Atun R. et al.
1
Atun, R.
1
Aubert P.
1
Auerbach, R.
1
August Burns, Linda O’Neal Eckert, Susan Hariri et al
1
Augustine, A.
1
AUNAIDS
1
Aung Zayar Paing
1
Aung, Toe Toe
1
Aurélie Davy, Solène Mérandon, Sandra Sladoljev
1
Austin-Evelyn K, Rabkin M, Macheka T, Mutiti A, Mwansa-Kambafwile J, Dlamini T, et al.
1
Australian Commission on Safety and Quality in Health Care (ACSQHC)
1
Australian Government AusAID
1
Australian Institute of Family Studies Child Family Community
1
Australian National Clinical Evidence Taskforce
1
Australian Women's Health Network
1
Avaria, A. et al.
1
Avi Kenny, Gaurab Basu, Madeleine Ballard et al.
1
Awoyemi Abayomi Awofalaa, Olusegun Emmanuel Ogundele
1
Awudu, RA.
1
Ayala, George
1
Ayalew, A. et al.
1
Aye Kyawt Paing et al.
1
Ayele, Wondimu, Habtamu Tesfaye, Roman Gebreyes, and Tesfayi Gebreselassie
1
Ayele, Wubegzier Mekonnen
1
Aziz N. A., S. S. Mohamed, T. A. Badara et. al.
1
Aziz, A.
1
Ärtze der Welt
1
Ärztliches Zentrum für Qualität in der Medizin
1
Åsa Hammar and Guro Årdal
1
B Watso, E.Togami et al.
1
B-Lajoie,MR. O. Drouin,G. Bartlett, et al.
1
B. Falissard
1
B. A. McCormick and R. J. Eltringham
1
B. Aracena-Genao
1
B. B. Bachore
1
B. Bandelow, L. Sher, R. Bunevicius, et al.
1
B. Birmaher
1
B. C. Zanoni
1
B. Cao
1
B. Chimukangara
1
B. Davis
1
B. Diaz
1
B. Durovnia
1
B. Ezenwa
1
B. Frank‐Hatitchki: O. Ogunwobi
1
B. H. Singer (Princeton University)
1
B. Hauer, R. Loddenkemper, A. Detjen, et al.
1
B. J. Mohapia
1
B. James, Ph.D.
1
B. K. Roy
1
B. Karo
1
B. Kollo
1
B. Konstantinov
1
B. M. McCoy
1
B. Mason Meier
1
B. Mboya, P. Maro, J. Gulaka et al.
1
B. Moges, B. Amare, F. Asfaw, et al.
1
B. N. Ezenwa, I. B. Fajolu, O. R. Akinajo, et al.
1
B. Noubary
1
B. Nurcombe
1
B. Ohye
1
B. O’Donnell
1
B. Parks et al.
1
B. Rajamaki
1
B. Refetllari
1
B. Russell et al.
1
B. S. Singhal
1
B. StamblerI
1
B. Subha Sri
1
B. Tesfaye
1
B. Unnikrishnan
1
B. Williams
1
B. Wolff, L. de Carlo
1
B. Xhani
1
B.Bandelo, S. Michaelis, D. Wedekind
1
B.Callender, V. Adams, et al.
1
B.de Mucio, et al.
1
Baard, C.B.
1
Baas, Stephan
1
Badan Nasional Penanggulangan Bencana
1
Baden-Württemberg Ministerium für Kultus, Jugend und Sport
1
Badrizadeh, A.
1
Baer B.
1
Baer,, U. und U. Harper
1
BAff
1
Bagattini AM, de Melo Tavares B, Garcia Moraes Pagano C, et al.
1
Bahar Oghalai
1
Bahiru, E.
1
Bakare, M.O., Ubochi, V.N., Ebigbo, P.O. and Orovwigho, A.O.
1
Bakiono F., Wendpouiré P., Guiguimdé L. et. al.
1
Balaji, V., P. Rupali, K. Walia, et al.
1
Balakasi, K.
1
Balamurali, M.
1
Balasegaram, M.
1
Ballot, Andreas
1
Balma, L.
1
Balmes, J.R.
1
BALSAM
1
Bamba S. , Zida A., Sangaré I. et al.
1
Bambrick, H.
1
BAMF
1
Banda, H.T. et al.
1
Bangladesh Institute of Development Studies (BIDS) Grantee
1
Bangladesh Nursing Council
1
Bangladesh Red Crescent Society , German Red Cross
1
Bangpan, M
1
Bapoutou, B.
1
Baptist, A.P.
1
Baral, P.
1
Baraldi, E.
1
Barasa, E.
1
Barasa, V.
1
Barba, E.
1
Barbara McPake, Ijeoma Edoka, Sophie Witter, et al.
1
Barben et al.
1
Barbosa Martelli, D. R.
1
Barcelos TN, Muniz LN, Dantas DM et al.
1
BardenO'Fallon J, Barry MA, Brodish P, et al.
1
Bardosh, K.
1
Barker, G.
1
Barnes, H.
1
Barráez, D.
1
Barrera l., Imaz M. S., et al.
1
Barrera-Valenciaa, M., Calderón-Delgado, L., Trejos-Castillo, E. & O’Boyle, M.
1
Barrett, M.P.
1
Barrios, R.N.
1
Barry A, Barden O’Fallon J, Hazerjian J, Brodish P
1
Bartlett, E. S.
1
Bartoloni, A.
1
Bashemera, Domitilla R., Martha J. Nhembo, and Grace Benedict
1
Basic Needs Ghana
1
BASICS
1
Basinga, P., Gertler, P.J., Binagwaho, A., et al.
1
Bastable, Andy and Russell, Lucy
1
Bataduwaarachchi, V.R.
1
Bateman, E. D.
1
Bateman, E.D.
1
Bath, D.
1
Batista, C.
1
Bauer, H.
1
Bauersachs, J.
1
Baxter, N.
1
Bay, N. et al.
1
Baya B., A. Sana
1
Bayadinova, J.A., Sardo, Higgins-Nogareda, V., Scott, J. & MacKinnon, B.
1
Bayão T.S., Cupertino M.C., Gomes A.P. et al
1
Bayerisches Landesamt für Gesundheit und Lebensmittelsicherheit
1
Bayerisches Staatsminiserium für Arbeit und Soziales, Familie und Integration
1
Bayerisches Staatsministerium für Gesundheit und Pflege
1
Bayerisches Staatsministerium für Umwelt und Gesundheit
1
Baylor International Pediatric AIDS Initiative (BIPAI)
1
Bayrisches Landesamt für Gesundheit und Lebensmittelsicherheit (LGL)
1
Bazargani, Y.T.
1
Bălă, G.P.
1
BBK
1
Beard, R. Suzanne
1
Beattie, T. K.
1
Beauftragte der Bundesregierung für Migration, Flüchtlinge und Integration Bundeskanzleramt
1
Becher, H.
1
Becker, A.
1
Beckman, M.
1
Beckmann, P.J.
1
Bedding, E.J.
1
Beer, J. de
1
Begum, Shazia
1
Begum, T. S. M.
1
Bekyol, Y.
1
Belkisyole Alarcón de Noya, Raiza Ruiz-Guevara, Zoraida Díaz-Bello, et al.
1
Belkum, A.van, T. T. Bachmann, G. Lüdke, et al.
1
Ben Naafs, et al.
1
Bendavid E. et al.
1
Benedetto Vitiello, Переводчик: Константин Мужановский
1
Benítez M. A., Martín E. P. S. et al.
1
Benjamin J. Park, MD
1
Benjamin O Alli [et al.]
1
Bennett, James et al.
1
Bennett. A., J. Yukich, M. Robertson, et al.
1
Benson Igboin
1
Benson-Martin, J.
1
Benton, T.
1
Benue State University, Nigeria
1
Beovic B., M. Dousak, C. Pulcini et al.
1
Berger, S.
1
Bergmann, J.
1
Berkley, James A.
1
Berkowitz, A.L.
1
Berlin, E.
1
Berliner, D.
1
Berman P.
1
Berman, D.
1
Bernal O, López R, Montoro E, et al
1
Bernal, O.
1
Bernard M. Branson, S. Michele Owen, Laura G. Wesolowski et
1
Bernd Rechel
1
Berry, P.
1
Bertozzi, Stefano
1
Best Care Always South Africa
1
Bethesda, MD: Health Finance & Governance Project, Abt Associates Inc.
1
Betrò, S.
1
Bettina B., J. Barnes, A. Carmona
1
Beverly D Glass
1
Bham A., J. Bhiman, F. Bongweni et al.
1
Bham, A.
1
Bhatnagar, A.
1
Bhattacharya A, et al.
1
Bhutta, Zulfiqar et al.
1
Biancovilli, p.
1
BIB Hounkpatin , Obossou AAA, Tonato-Bagnan A, Hounkponou FN, Aboubakar M, Sehlouan C , Tshabu Aguemon C, Sidi IR, Salifou K, Vodouhe MV, Perrin RX
1
Biccard, B.M.
1
Bickenbach, J., Cieza, A., Rauch, A. & Stucki, G.
1
Biddle, L.
1
Biedron, C.
1
Biessels. G.J. et al.
1
Bigna J. J., M.A. Amougou
1
Bigoni, A.
1
Billing T.
1
Bing Lin A. B., M.L Dietrich, R.A.Senior, et al.
1
Binyaruka, P.
1
Bio Med Central
1
Bioethics
1
Bioline international
1
BioMed Research International
1
Bischöfliches Hilfswerk MISEREOR, Brot für die Welt, Global Policy Forum
1
Bishop, G.
1
Bixby, H.
1
Bizimana, T.
1
BJOG An International Journal of Obstetics and Gynaecology
1
BKK Landesverband Bayern
1
Blaise Adelin Tchaou, Nouessewa Fanny Maryline Hounkponou Kabibou Salifou, Eugène Zoumenou, Martin Chobli
1
Blanc, P.D.
1
Blanco D.B.
1
Blocher, J.
1
Bloom, Barry R.
1
Bloomberg Philatrhopies, IFAG
1
Blum, JA.
1
BMA
1
BMC - Biomed Central
1
BMC Biology
1
BMC Cardiovascular Disorders
1
BMC Health Services
1
BMC Health Services Research, part of Springer Nature
1
BMC International Health and Human Rights
1
BMC Medical Education
1
BMC Pregnancy and Childbirth
1
BMJ Global Health Journal
1
BMJ Innovations :234–239. doi:10.1136/bmj
1
BMJ Open Respiratory Research
1
BMJ Open Science
1
BMZ
1
Bo Peng , Rowland W. Pettit, and Christopher I. Amos
1
Bo Wen, Rongbin Xu, Yao Wu, Micheline de Sousa Zanotti Stagliorio Coelho et al.
1
Board on Global Health
1
Board on Health Sciences Policy
1
Bodeker, Gerard (Ed.)
1
Bodeker, Gerard, Ong, Chi-Keong, Grundy, Chris, Burford, Gemma, Shein, Kin. et al. (2005). WHO global atlas of traditional, complementary and alternative medicine. Kobe, Japa
1
Bodenz, A.
1
Boeuf, P.
1
Bogousslavsky, J.
1
Bois et forêts des tropiques
1
Bolivia, Ministerio de Salud, Gobierno de Estado Plurinacional s
1
Bonelli, R.
1
Bonita, R.
1
Bont, L. et al.
1
Boogard, H.
1
BooMed Central
1
Borgeson, J. R.
1
Borghi, J.
1
Borghi, J. et al.
1
Borlase, A.
1
Bortone, B.
1
Bosede Abidemi Tella, Caleb Ademola Gbiri, Oluwaseyi Abigail Osho, A E Ogunrinu
1
Boston Consulting Group
1
Bosu, WK
1
Bouchaud O., C. T. Ndour et al.
1
Bouley, T. A.
1
Bouman, D., W. Novalia, P. Hiemstra, et al.
1
Bousquet, P.
1
Bovet, P.
1
Bower, J.
1
Boyce, M.
1
Börjesson, E., Pedersen, K., & Villa Torres, L.
1
Braam, D.
1
Brabin, L.
1
Bracho C., Martinez C. et al.
1
Bradleya, M.
1
Bradshaw, C.
1
Brady, O. J. et all.
1
Brain Sciences
1
Braitstein, Paula et al.
1
Brand, P.L. et al.
1
Brandon A. Kohrt,Laura Asher, Anvita Bhardwaj, et al.
1
Brazilian Journal of Health Review
1
Breastfeeding Foundation of Life
1
Breathe
1
Breathe, part of the European Respiratory Society (ERS)
1
Brehm, M
1
Breitegger, Alex
1
Breitner-Busch, S.
1
Brett D. Nelson, Maya Fehling, Margaret E. Tierna, Zina Maan Jarrah
1
Briegel, J.
1
Brindha, J.
1
Brindley, P. et al.
1
British Association for Cardiovascular Prevention and Rehabilitation
1
British HIV Association
1
British Medical Journal (BMJ)
1
Brittain, Kirsty et al.
1
Brocklehurst C.
1
Brockmeyer, B.
1
Broeckaert, B.
1
Brooks,J.T.
1
Brot für die Welt, Forum Umwelt und Entwicklung, Unfairtobacco, Global Policy Forum, Bischöfliches Hilfswerk Misereor
1
Brown C.M., Slavinski S., Ettestad P. et al
1
Brown S.
1
Brown, D.A.
1
Brown, J.
1
Brown, J.PR.
1
Brown, M.E.
1
Brown, T.
1
Brozek, J. L.
1
Bruniea, A.
1
Brunn, B.
1
Bruno Martorano, Laura Metzger, Marco Sanfilippo
1
Bruun, B.
1
Brymer M., Taylor M., Escudero P., Jacobs A., Kronenberg M., Macy R., Mock L., Payne L., Pynoos R., & Vogel J.
1
Buckley, A.
1
Buckley, P.
1
Budde, H.
1
Budreviciute, A.
1
Buendía, J.
1
Buffel, O.
1
Bui, B., Ohye, B., Palitz, S., et al.
1
Buissonniere, M.
1
Bukachi, SA.
1
BUKO Pharma-Kampagne/Gesundheit und Dritte Welt e.V.
1
Buliva E., Elnossery S., Okwarah P. et al.
1
Bundes-Psychotherapeuten-Kammer
1
Bundesfachverband unbegleitete minderjährige Flüchtlinge
1
Bundesfachverband unbegleitete minderjährige Flüchtlinge BumF
1
Bundesfachverband Unbegleitete Minderjährige Flüchtlinge e.V.
1
Bundesinstitut für Arzneimittel und Mediziprodukte
1
Bundesministerium für wirtschaftliche Zusammenarbeit und Entwicklung BMZ
1
Bundesverband für körper- und mehrfachbehinderte Menschen e.V.
1
Bundesvertretung der Medizinstudierenden in Deutschland BVMD
1
Bundesvertretung der Medizinstudierenden in Deutschland e.V.
1
Bundesweite Arbeitsgemeinschaft der Psychosozialen Zentren für Flüchtlinge und Folteropfer – BAfF e.V.
1
Bundesweite Arbeitsgemeinschaft der Psychosozialen Zentren für Flüchtlinge und Folteropfer – BAfF e.V
1
Bundesweite Arbeitsgemeinschaft der psychosozialen Zentren für Flüchtlinge und Folteropfer
1
Bundesweite Arbeitsgemeinschaft der Psychosozialen Zentren für Flüchtlinge und Folteropfer (BAfF e.V.)
1
Bundesweite Arbeitsgemeinschaft der psychsozialen Zentren für Flüchtlinge und Folteropfer BAfF
1
Bundeszentrale für gesundheitliche Aufklärung (BZgA)
1
Bundeszentrale für gesundheitliche Aufklärung BZgA
1
Bundy, Donald A. P.
1
Bunning K, Gona JK, Newton CR, Hartley S
1
Bureau régional de l’OMS pour l’Afrique
1
Burns, A. and S. Iliffe
1
Burns, J.
1
Burrone M. S., Reginatto G. et al
1
Burt Perrin
1
Burton Blatt Institute at Syracuse University and the Secretariat for the Convention on the Rights of Persons with Disabilities, UNDESA
1
Burton, A.
1
Bush, A.
1
Busquets, J.
1
Buss, K.E., Warren, J.M. & Horton, E.
1
Bustamente, J. Teleducacion Facultad de Medicina Universidad de Antioquia
1
Butkus, R. A.
1
Bwalya, Bupe B., Mulenga C. Mulenga, and James N. Mulenga
1
by Mark Nunn, Annalies Borrel, Allison deFranco et al.
1
By the Committee on Ethical Aspects of Human Reproduction and Women's Health, International Federation of Gynaecologists and Obstetricians (FIGO)
1
BZgA
1
C G. Alvarenga Cardoza, K.M. Díaz de Naves
1
C Ip, E.
1
C.
1
C. Kouambeng, R. Wounang et. al.
1
C. Soutullo
1
C. A. Bernad
1
C. Acevedo
1
C. Aguilera
1
C. and B. Kwagala
1
C. Beecroft
1
C. Benedikt
1
C. Beurenmeister, A. K. Birkenstock, Brenner J., et al.
1
C. Beyrer
1
C. Breuer
1
C. C. Chakanyuka Musanhu al.
1
C. C. Onyedum, I. Alobu, K. N. Ukwaja
1
C. Cappa, N. Petrowski , J. Njelesani
1
C. Celum
1
C. Centeno, Sitte, T. de Lima L. et.al.
1
C. Clift
1
C. Contini, M. Maritari, M. die Nuzzo, et al.
1
C. Cravero, S. Danner et. al.
1
C. D. Chikwari
1
C. D. Mitchell
1
C. DC Christie-Samuels
1
C. Dias Azevedo, G. Fernandes Maciel da Silva et al.
1
C. Diehl, B. Leyendecker
1
C. Fitzpatrick, J.Jannin
1
C. Folch
1
C. Freeman
1
C. Giannou and M. Baldan
1
C. Giannou, M. Baldan and A. Molde
1
C. Glazebrook
1
C. Green
1
C. Grollman
1
C. Hanlon, A. Alem, C. Lund, et al.
1
C. Hasenkopf and K. Lee
1
C. Hoffmann und J. K. Rockstroh
1
C. Hoffmann, A. Gualani Gualani
1
C. Hoffmann, et al.
1
C. Hoy, and E. Ortiz-Juarez
1
C. Hughes
1
C. J. Berg
1
C. J. Schellack
1
C. K. Mbuba
1
C. Kanabkaew
1
C. Kennedy
1
C. Kieling
1
C. Kollan
1
C. L. Katz
1
C. L. Moore
1
C. Leopold
1
C. M J E Vandenbroucke-Grauls, G. Kahlmeter, J. Kluytmans et al.
1
C. M. Yuen, H. O. Weyenga, A. A. Kim, et al.
1
C. MacNamara, L. Varley, P. M. McNamara
1
C. Martinez
1
C. McMichael
1
C. Mihalopoulos
1
C. Mpody, et al.
1
C. Murendo
1
C. Murray
1
C. Nkoke
1
C. Oliveras
1
C. Oprea
1
C. Opreab
1
C. P. Fernández
1
C. P. Salvo, P. Kuschner, et al
1
C. Pasquini
1
C. Perplies
1
C. Pettitt-Schieber, M. Owen, et al.
1
C. Pérez Casas
1
C. Pitt
1
C. Quinn
1
C. R. Newton
1
C. R. Vitek
1
C. Rae
1
C. Redick
1
C. Rodgers
1
C. Rooney
1
C. S. Biskup
1
C. S. Biskup, Martin Holtmann
1
C. S. Yaha
1
C. Savolainen-Kopra
1
C. Soutullo
1
C. Thomson
1
C. Thuman and J.Maxwell
1
C. Torres and F. Rampa
1
C. Victora and M. Chowdury.
1
C. Walter V.
1
C. Weiß and M. Wehling
1
C. Wilcox, L. Lebreton et al.
1
C. Workman
1
C.A.Faerron-Guzman
1
C.Bachmann
1
C.Heydenreich und S.Lincoln
1
C.P.
1
C.Stefan, F. Bray, J. Ferlay, et al.
1
C.Victor
1
C.Walter V.
1
CAAP12
1
Cad. Saúde Colet.
1
Cadena-Gaitán, C.
1
Cadernos de Saúde Pública
1
Cafasso, J.
1
CAFOD
1
Cairn Info
1
Cairn info - chercher, répéter, avancer
1
Calcagno, J.
1
Caldas de Almeida, José Miguel (ed.) & Cohen, Alex (ed.).
1
Calitz, F.J., de Jongh, N.J., Horn, A., Nel, M.L. & Joubert, G.
1
Calligaro, G.
1
Calverton, Maryland, USA: ICF International.
1
Cama, V. et al.
1
Cambodia, Ministry of Health, PMNCH, WHO, World Bank, AHPSR et al.
1
Camp, O.
1
Camp, R. and C. Hoffmann
1
Campbell Collaboration
1
Campbell J.
1
Campbell, L
1
Campbell, L.
1
Campero A.
1
Campos de Meli Iani, F.
1
Campos Vieira Abib, S.de
1
Campos, A.
1
Canadian Association of Physicians for the Environment (CAPE)
1
Canadian Psychological Association
1
Canadian Red Cross
1
Cancer
1
Cancer Medicine
1
CANSA
1
Cao-Lormeau VM, Blake A, Mons S, Lastère S, Roche C, Vanhomwegen J, Dub T, Baudouin L, Teissier A, Larre P, Vial AL, Decam C, Choumet V, Halstead SK, Willison HJ, Musset L, Manuguerra JC, Despres P, Fournier E, Mallet HP, Musso D, Fontanet A, Neil J, Ghawché F
1
CAP-China
1
Capacity Project
1
Caparrós-Martínez J.L., Rueda-López N., et al.
1
Cappa, C.
1
Capps, B.
1
Caqueo-Urízar A., Urzúa A. et al
1
Caran Ann, M.
1
Carbonell, C.
1
Cardiovascular Research
1
CARE International
1
Care, et al.
1
Carine Baxerres
1
Caritas Würzburg, Landkreis Würzburg
1
Caritas, et al.
1
Carla Cabral dos Santos Accioly Lins
1
Carla Silva-Matos
1
Carlier, Y.
1
Carlo Oliveras
1
Carmen de Witt-Amrein
1
Carol Taylor & Catherine Aldred
1
Carolina L.A. Barbieri, C. Carvalho de Souza Amorim Matos
1
Caroline Hickman, Elizabeth Marks, Panu Pihkala et al.
1
Carrillo-Larco
1
Casa
1
Cassola, A.
1
Castillo C., Villalobos Dintrans P. et al
1
Castro, A.
1
Castro,, P.
1
Catherine O Egbe, C.Brooke-Sumner†, T. Kathree,et al.
1
Catholic Relief Services (CRS) & Hilton Foundation
1
Cavallaro F. L., L. Benova, D. Macleod et. al.
1
CAWST Centre for Affordable Water and Sanitation Technology
1
Cawthrope, D.
1
CBM East Africa Regional Office
1
CBR Africa Network, Handicap International
1
CBR Asia-Pacific Network
1
CDC Centers for Disease Control and Prevention
1
CDC et al.
1
CDI&PRH, FIRA, Centre Ressource
1
Cecchi, G.
1
Cecchini, M.
1
Cecil Konijnendijk, Dikshya Devkota, Stephanie Mansourian & Christoph Wildburger (eds.)
1
Center for Strategic & International Studies CSIS
1
Center for Disease Control
1
Center for Disease Control and Prevention
1
Center for Disease Control and Prevention, World Health Organisation
1
Center for Global Development
1
Center for Public Interest Communications, University of Florida
1
Centers for Disease Control
1
Centers for Disease Control & Prevention
1
Centers for Disease Control and Prevention , World Health Organization WHO
1
Centers for Disease Control and Prevention CDC, American Nurses Association ANA
1
Centers for Disease Control and Prevention, National Center for HIV
1
Centers of Disease Controle CDC
1
Central Asia-Caucasus Institute
1
Central Leprosy Division
1
Central Research Institute of Epidemiology of Rospotrebnadzor
1
Central TB Division Ministry of Health and Family Welfare, Government of India
1
Central TB Division, Director ate General of Health Services, Ministry of Health & Family Welfare
1
Central TB Division, Directorate General of Health Services, Ministry of Health & Family Welfare, Nirman Bhavan
1
Central TB Division, Directorate General of Health Services, Ministry of Health & Family Welfare
1
Centre Anti Poison du Maroc
1
Centre d'Estudis Epidemiològics sobre les Infeccions de Transmissió Sexual i Sida de Catalunya (CEEISCAT)
1
Centre d’Information Pharmacothérapeutique du Bénin (CIP-BENIN)
1
Centre for Addiction and Mental Health (CAMH)
1
Centre for Antibiotic Resistance Research (CARe), University of Gothenburg
1
Centre for Disability Studies, NALSAR University of Law Hyderabad
1
Centre for Health Protection
1
Centre for Heath & Infectious Disease Research
1
Centre for Human Rights Promotion – CHRP
1
Centre for International Health and Development
1
Centre for Maternal and Newborn Health (CMNH), from the Liverpool School of Tropical Medicine (LSTM)
1
Centre for Renewable and Sustainable Energy Studies (CRSES) at Stellenbosch University
1
Centre for Respiratory Diseases and Meningitis and Outbreak Response
1
Centre Pasteur du Cameroun
1
Centros africanos para el control y la prevención de enfermedades El Centro de Dinámica de Enfermedades, Economía y Política
1
Centrul Naţional de Management în Sănătate
1
Cepuch, C.
1
CERAH
1
Cercone, James
1
Cerda A. A., Garcia L. Y.
1
Cerebral Palsy Alliance Research Foundation
1
Cerveny, R. et al.
1
Cesare, M.D.
1
CG Working Group, Child Lung Health Section, International Union Against Tuberculosis and Lung Disease
1
CGIAR
1
Chaitkin, Michael
1
Chaitra Gopalappa, John Stover & Carel Pretorius
1
Chakane, Ntema
1
Chakaya, J.
1
Chalasani, Sativika
1
Challenge TB
1
Chambliss, S. E.
1
Chana, R
1
Chandani, Y.
1
Chang Campos, C.
1
Chang, Judy et al.
1
Chang, S.W.
1
Channel Research
1
Chansa, C.
1
Chapotera, Gertrude, Vinitha Jayachandran, and John Phuka
1
Charité Berlin
1
Charles B. Nemeroff
1
Charles I Azih
1
Charles Phiilipe de Lucena AlvesJoão de Deus Barreto Segundo, Gabriel Gonçalves da Costa et al.
1
Charlotte Feldman-Jacobs, et al.
1
Charlson, F.J.
1
Chas J., Hema A., Slama L. et. al.
1
Chatham House
1
Chattopadhayay-Dutt, Purnima
1
Chaturaka Rodrigo, Tharanga Fernando, Senaka Rajapakse, et al.
1
Chaud, P.
1
Chauhan, A. P.
1
Chavan, B. S.
1
Chayn
1
Chaziya J, Freyne B, Lissauer S et al.
1
Checchi F.
1
Chee H. Ng
1
Cheesbrough, M.
1
Cheesbrough, Monica
1
Chelo D., Kinkela M.N., et.al.
1
Chen Shen, Nan Xia, et al.
1
Chen, Y.
1
Cherrie Evans
1
Chetty, S.
1
CHF International, USAID
1
Chhea, Chhorvann, Por Ir, and Heng Sopheab
1
Chiara Servili, Juliana Yartey, M.T. Yasamy, et. al.
1
Chidebe, R.C.W., and M.L. Pratt-Chapman
1
Chikutsa, Antony, Alfred C. Ncube, and Shepard Mutsau
1
Chikwasha, Vasco, Isaac Phiri, Pugie Chimberengwa, Donewell Bangure, and Simbarashe Rusakaniko
1
Child Trends
1
Children Research Centre
1
Children's HIV Services (Be their key to life)
1
Children’s Health Policy Centre
1
Chimimba, F.
1
China CDC Weekly, CCDC Weekly
1
China-Japan Friendship Hospital
1
Chinenye Anyanwu, E.
1
Chintsanya, Jesman
1
Chiolero, A.
1
CHIP
1
CHIPER (Paediatric HIV matters)
1
Chipungu, C.
1
Chiriac, D.
1
Chitereka, J., P. Mandikutse, D. Nguo, N. Sithole, and N. Madzingira
1
Chochrane Library
1
Choon Guan Lim, Hannah Loh, Vidhya Renjan, Jason Tan and Daniel Fung
1
Chou-Zen Giam
1
Chowdhary, N.
1
Chowell and Nishiura
1
Chris Naylor
1
Christa L Fischer Walker, Igor Rudan, Li Liu, Harish Nair, et al.
1
Christie, I.
1
Christina Brandes-Barbier, Véronique Millot, Tomas Allen et al
1
Christoffel-Blinden Mission (CBM)
1
Christophe Peyrefitte
1
Christopher J. M. Whitty, Jeremy Farrar, Neil Ferguson, W. John Edmunds, Peter Piot, Melissa Leach & Sally C. Davies
1
Christopher J.L. Murray1 & Julio Frenk
1
Chu, D.K.
1
Chua, P.L.C.
1
Chukwu, E., Oladele, D., Awoderu, O. et al.
1
Chung, K. F.
1
Ciais, P.
1
Cianconi, P.
1
CICV, et al.
1
CIES IUL
1
Cifuentes, R-
1
Cilliers, J.
1
Cindil Redick& annah Sarah Faich Dini
1
Circulation: Heart Failure
1
Civil Society Alliance for Nutrition, Nepal (CSANN)
1
Clare Gilbert
1
Clarence J. Peters
1
Claritas Journal
1
Clark M.J.,
1
Clark, A.M. et al.
1
Clark, J.
1
Clarke-Deelder, E., G. Shapira, H. Samaha, et al.
1
Claudia Hanson, Jonathan Cox, Godfrey Mbaruku, et al.
1
Clayton J.
1
Clayton O. Onyango, Regina Njeru, Sidi Kazungu et al.
1
Clear Waters from Pharmaceuticals (CWPharma)
1
Cleary A. , Braubach M.
1
Clift, Jack
1
Climate Central
1
Clinica lResearch Unit for Anxiety Disorders, Sydney
1
Clinical Info HIV
1
Clinical Info HIV gov.
1
Clinical Microbiology Reviews
1
Clinical Nurse Specialist – Tissue Viability
1
Clinics in Mother & Child Health
1
Clinton Health Access Iniative
1
Clínica Universitaria Psicología
1
Clouse, Emily
1
Cloutier, M. M.
1
CMAM
1
Cobrales, M.
1
COC Netherlands
1
Cochrane
1
Cochrane Convenes
1
Cochrane Database of Systematic Reviews
1
CODEVIDA, Coalición de Organizaciones por el Derecho a la Salud y a la Vida
1
Cogent Medicine
1
Cohen, A., Eaton, J., Radtke, B., et al.
1
Cohen, A.J.
1
Cohen, R., Sharonann, L., Bygrave, H., et al
1
Cole CP, James PB, Kargbo AT
1
Cole, M.J.
1
Colin Cook, Babar Qureshi, Harpreet Kapoor, Dominic Misquith, and David Lewis
1
Colin Robson & Peter Evans
1
COLL-SECK, A. M.
1
College of American Pathologists
1
College of Nurses of Ontario
1
Collin F. Payne and Hans-Peter Kohler
1
Collins, T.E.
1
Colloquium on the International Protection of Refugees
1
CollSeck,A.M.
1
Colón-González, F.J.
1
Colston, J.
1
Columbia University, IFRC, Protection Cluster, et al.
1
Combary, P., Sinzahera, J., Mukakarara, V., et al.
1
Cometto, G.
1
Comic Relief
1
Comité Africain d’Experts sur les Droits et le Bien-être de l’Enfant CAEDBE
1
Comité internacional de la Cruz roja
1
Comité international de la Croix-Rouge (CICR)
1
Commonwealth Health Partnerships
1
Communicable Disease Control Branch - Manitoba Health
1
Communicating with Disaster Affected Communities (CDAC)
1
Community Development Medicinal Unit
1
Community Ear & Hearing Health
1
Community Eye Health
1
Community Health Services Unit
1
Community Health Services Unit, Ministry of Health, Department of Nutrition, HIV and AIDS Lilongwe, Malawi
1
Compaign for tobacco-free Kids
1
Conant , J.
1
Conciliation Resources
1
Condo J, et al.
1
Confederación Boliviana de la Persona con Discapacidad
1
Conférence épiscopale allemande sur les affaires internationales de l'Eglise
1
Coninx, R.
1
Conlon C., T. McDonnell, M. Barrett, et al.
1
Connolly, M.A.
1
Conseil Européen de Réanimation
1
Conseil International des Infirmières
1
Consejo interncional de enfermeras
1
Consejo Nacional de Evaluación de la Política de Desarrollo Social (CONEVAL)
1
Conselho Nacional de Combate ao HIV e SIDA (CNCS)
1
Conselho Nacional de Combate ao HIV e SIDA , Moçambique
1
Consorcio Latinoamericano de Anticoncepción de Emergencia (CLAE), Naciones Unidas, et al.
1
Consortium for Universities for Global Health
1
Conteh, L. et al.
1
Convention on Biological Diversity
1
Cook B.
1
Cooper et al. BMC Medicine
1
Cooper, C. M.
1
Cooper, P. J.
1
Coordinación Nacional de Hepatitis Virales
1
Coordinating Minister of People's Welfare
1
Corbett, E. L.
1
Cordaid
1
Cordeiro Jardim, B.
1
CORE Group
1
CORE Group, Save the Children, BASICS et MCHIP,
1
Corella de Sousa, J.
1
Corfmat, J.
1
Corinne Grainger
1
Corman, V.
1
Cornick, Picken, Wattrus et al.
1
Correia de Sousa, J. et al.
1
Corum, J.
1
Corvalan, C.
1
Cosgrave, J.
1
Cossi Angelo Attinsounon, Comlan Albert Dovonou, René Kèkè, Cossi Adébayo Alassani, Kouessi Anthelme Agbodandé, Finagnon Armand Wanvoegbe, Angèle Kouanou-Azon, Djimon Marcel Zannou
1
Costa Kazadi Mwadianvita et al. The Pan African Medical Journal
1
Costa, F.
1
Cottani, J.
1
Cotton, M., et al.
1
Couldrey, M.
1
Coulibaly M., N. Meda, C. Yonaba et al.
1
Coupland, R
1
Coupland, Robin M.
1
Couto,M.T.
1
COVID-19 Mental Disorders Collaborators
1
Covill, N.
1
Cowater
1
Cowl, C.T. et al.
1
Cowling K.
1
Cox, Jonathan
1
CRA Terre
1
Crane, J.
1
Crane, M.
1
Crawford E., Suvedi M.
1
Crofts, K.
1
Crosbie, E.
1
Cubillos-Novella A., I. Bojorquez-Chapela, J. A. Fernandez-Nino
1
Cucunubá Z.M., Valencia-Hernándeza C.A. , Puerta C.J. et al
1
Cucunubá, Z.
1
Cullinan, P.
1
Cullinane P.J.
1
Cupertino, M. C.
1
Cupp, E.
1
Curatio International Foundation
1
Curationis
1
Cureus
1
Current Opinion in Psychiatry
1
Current Tropical Medicines Report
1
Currier, J.S.
1
Curry International Tuberculosis Center, State of California, California Health & Human Service Agency, Department of Public Health
1
Cyril Caminade, Sari Kovats, Joacim Rocklov et al.
1
D. Acosta
1
D. Antognini, A. Combes, et al.
1
D. B. Garfinkel
1
D. Bajpai
1
D. Breuer
1
D. C. Etal
1
D. Carr
1
D. Chisholm
1
D. D. Bui
1
D. Daniels
1
D. Daniels, C. Smyth, et al.
1
D. Daniels, et al.
1
D. de Lange
1
D. de Lange, D. Radeloff
1
D. Dufour
1
D. Evans
1
D. Fitzgerald, U. Terblanche and K. Kritzinger
1
D. Ford
1
D. Fung
1
D. Gamboa et al.
1
D. Giacco, and Rawda El-Nagib.
1
D. Gokengina,
1
D. Gomez-Pastrana
1
D. Gökengin
1
D. Grace
1
D. Grant
1
D. Gyamfi Amoako, R. Carrel Founou, et al.
1
D. H. Mulligan,
1
D. Hedrich
1
D. Hirschland
1
D. J. Jackson
1
D. Jamieson
1
D. K. de Souza
1
D. Kerrigan
1
D. Liriope
1
D. Low-Beer
1
D. Luo
1
D. Maradiaga
1
D. Mathiot
1
D. Mueller et al.
1
D. O. Frauches
1
D. Ocheret
1
D. Otiashvili
1
D. O’Mahony
1
D. P. Chin, C. L. Hanson
1
D. Peyramond, C. Rapp, H. Coignard, et al
1
D. Purnamasari, S. Waspadji, J. MF Adam, et al.
1
D. Ramos
1
D. Ruiz
1
D. S. Nsagha
1
D. Stuckler, S. Basu, M. McKee, et al.
1
D. Susanty
1
D. Tappe, C.Kasang, A. Mueller
1
D. Todt, P. V’kovski, et al.
1
D. van der Veur
1
D. Wolfe
1
D. Yu
1
D.Cavil, S. Musyoki, et al.
1
D.Currie
1
D.de Lange
1
D.E.
1
D.enis Akakimpa
1
D.L. Richards, C. Campbell, A. Adams, S. Fantahun, K. Layne
1
D.L. Terlonge
1
D.M. Bowley, et al.
1
D.M. Iwaniec, T. McPhearson
1
D.Walker
1
Daalen, K.R. van
1
Dabiré J. Y.
1
DAC Network on Conflict, Peace and Development Co-operation and DAC Network on Development Evaluation
1
Dacombe R., I. Bates, B. Gopul et al.
1
Dadvand, P.
1
Dahab M.
1
Dahal P., Bhattarai B., Adhikari D., et al.
1
Dai, W., Kaminga, A.C., Tan, H., Wang, J., Lai, Z., Wu, X., Xiong, Y., Deng, J. & Liu, A.
1
Dalla Lana School of Public Health, University of Toronto
1
Dalutira, G.D.
1
Damialis, A.
1
Damiati, S.
1
Dan Chisholm, Kim Sweeny, Peter Sheehan, et al.
1
Dan Hanfling, John Hick, and Clare Stroud
1
Daniel Mont
1
Daniel S. Chertow, Christian Kleine, Jeffrey K. Edwards, Roberto Scaini, Ruggero Giuliani, and Armand Sprecher
1
Daniele M.A., Ganaba R., Sarrassat S. et. al.
1
Danish Red Cross
1
Danish Refugee Council, Norwegian Refugee Council, CARE, et al.
1
Danyuttapolchai, J., S. Kittimunkong, S. Nateniyom, et al.
1
Dar M J
1
Darika Saingam
1
das Neves Martins Pires P.H. , Macaringue C. , Abdirazak A. et al.
1
Dasandi, N.
1
DATER House
1
Datta, B. et al.
1
Datta, B.K.
1
Daudt, H. et al
1
Daures, J.
1
Dave, R.
1
David Beran
1
David Bonbright, Keystone Accountability
1
David Fishman
1
David Lewis and Kath Ballard
1
David Lloyd Roberts
1
David Marsh, Ashley Aakesson, Kechi Anah et al.
1
David P.M., Le Dévédec N. et al.
1
David Sanderson and Ben Ramalingam
1
David Sanderson and Paul Knox-Clarke
1
David. M. Ndetei
1
Davies, J.S.
1
Davies, T.
1
Davis, Bill
1
Davis, Ian
1
Davis, J.
1
Day S., Challinor J., Hollis R., et al.
1
De Beni, Davide
1
de Ferrari, A.
1
de JOng, L.
1
de Jong, T.
1
De Jongh T.
1
De la Porte, A.
1
de Man P, van den Dobbelsteen J, et al.
1
De Neve. J.-E.
1
de Silva, Nilanthi
1
de Vries D, Blair G, Morgan K
1
Dear J.
1
Debas, Haile T.
1
Debbie DeVoe
1
Dedford, C.
1
Defensoria Pública do Estado de São Paulo
1
DeFilipps, Robert A.
1
Delia Grace
1
Delia Saldaña
1
Deliver
1
Delphine Boulenger, Basile Keugoung & Bart Criel, Institute of Tropical Medicine, Antwerp
1
Delphine Sculier, Haileyesus Getahun, Reuben Granich
1
Democratic Socialist Republic of Sri Lanka
1
Denis Mubiru, Robert Byabasheija, John Baptist Bwanika, et al.
1
Denise Razzouk , Guilherme Gregório, Renato Antunes, Jair de Jesus Mari
1
Dennis Falzon, Elizabeth Harausz, Ernesto Jaramillo et al.
1
Dennis, C.
1
Deogratias Mazigo, H.
1
Depar tment of Health, National Center for Disease Prevention and Control
1
Departamento Alimentos y Nutrición División Políticas Públicas Saludables y Promoción
1
Departamento de Gestão e Incorporação de Tecnologias e Inovação em Saúde – DGITIS
1
Departemen Kesehatan Republik Indonesia
1
Department for International Development DFID
1
Department for International Development (DFID)
1
Department of Education, Republic of South Africa
1
Department of Essential Medicines and Health Products (EMP) and NVI
1
Department of Health & Department of Basic Education, Republic of South Africa
1
Department of Health & Human Services
1
Department of Health & Human Services USA
1
Department of Health (DOH)
1
Department of Health (DOH), Republic of the Philippines
1
Department of Health and Human Services - USA
1
Department of Health Research Ministry of Health & Family Welfare
1
Department of Nutrition
1
Department of Public Health, Ministry of Health, Gabarone, Botswana
1
Department of Reproductive Health and Research
1
Department Soziales und Gesundheit Kanton Aargau
1
Department: Agriculture, Foresty and Fisheries - Republic of South Africa
1
Department: Health Republic of South Africa
1
Departments of Health and Agriculture, Forestry and Fisheries for the Republic of South Africa
1
Dept of Agriculture, Forestry & Fisheries, South Africa
1
Dept. of Health
1
Dept. of Health South Africa
1
Dept. of Pediatrics, All India Institute of Medical Science, New Delhi, India
1
Dept. of Psychiatry
1
Dept. of Women and Child Health Development, India
1
Depto. Ciclo Vital División Prevención y Control de Enfermedades
1
Der Paritätische Gesamtverband
1
Derek Summerfield
1
Dermatol Venez
1
Dermatol Venez, Univerisdad Central de Venezuela
1
Dermot Maher
1
Desclaux A., O. Ky-Zerbo, J.-F. Somé et. al.
1
Desogus, A.
1
Detges, A.
1
Detjen A, Gnanashanmugam D, Talens A
1
Deutsche Forschungsgemeinschaft
1
Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin e.V.
1
Deutsche Gesellschaft für International Zusammenarbeit (GIZ)
1
Deutsche Gesellschaft für Internationale Zusammenarbeit (GIZ)
1
Deutsche Gesellschaft für Internationale Zusammenarbeit GmbH (GIZ)
1
Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ) GmbH
1
Deutsche Gesellschaft für Tropenchirurgie
1
Deutsche Platform für Global Gesundheit DPGG
1
Deutsche Welthungerhilfe e.V.
1
Deutschen Gesellschaft für Tropenmedizin und Internationale Gesundheit (DTG) in Zusammenarbeit mit der Paul-Ehrlich-Gesellschaft für Chemotherapie (PEG) und der Deutschen Dermatologischen Gesellschaft
1
Deutscher Bundestag
1
Deutscher Verein für öffentliche und private Fürsorge e.V.
1
Deutsches Ärzteblatt International
1
Deutsches Institut für Menschenrechte
1
Deutsches Zentralkomitee zur Bekämpfung der Tuberkulose
1
Development Initiatives Poverty Research Ltd.
1
Development of Health and Human Services USA
1
Development Pathways
1
Development Studies Network
1
Developmental Epidemiology Program
1
Devipriya, J.
1
Devlin, K.
1
Dey de Pryck, Jenny et al.
1
DEZA Direktion für Entwicklung und Zusammenarbeit
1
Dèdonougbo Houenassi, M.
1
DFID (Department for International Development)
1
DGS
1
DGVS
1
Dhan Bahadur Shrestha, Pravash Budhathoki, Bipana Gurung et al.
1
Dhara Thakar
1
Dharini Bhuvanendra
1
Dheda, K.
1
DHHS Publication
1
DHS Further Analysis Reports No. 111
1
Diabete Care
1
Diabetes & Metabolism Journal
1
Diabetes Internacional
1
Diabetes Internacional y endocrinología
1
Diabetes Internacional, Universidad Central de Venezuela
1
Diabetes Research and Clinical Practice
1
Diadié Maïga, Bedel Evi, Angélique Gbaguidi
1
Diagnostics Technical Advisory Group (DTAG)
1
Diallo A. B., A. I. Kollo, M. Camara et. al.
1
Diallo A., D. L. Dahourou, T. T. E. Dah et al.
1
Diana P. Rojas-Alvarez
1
Diarra, A. et al.
1
Dib, J.
1
Dibb-Fuller, E, T. Liversedge
1
Dickie, E.A.
1
Die Sternsinger - Kindermissionswerk
1
Diego J. Rodriguez, Matthijs Schuring, Nansia Constantinou et al.
1
Diego Santana, Patricia Castellanos, Siân Tesni
1
Diel, R., G. Loytved, A.Nienhaus, et al.
1
Dieleman, J.
1
Dielmann J.
1
Dieng, Y. B. Faye, D.Ndiaye
1
Differentiated service delivery
1
DIFID
1
Diggins, J.
1
Dilys Morgan, Hilary Kirkbride and Bengü Said
1
Dimala, C.A.
1
Dingle, A.
1
Diono, Agus
1
Diouf A., T. J. Youbong, F. L. Dieye et. al.
1
Dirección de Medicamentos y Tecnologías en Salud, Colombia
1
DIRECCIÓN GENERAL DE SALUD PÚBLICA, CALIDAD E INNOVACIÓN
1
Dirección Nacional de Atención Pre-hospitalaria y Unidades Móviles, Ecuador
1
Direction de la lutte contre la maladie, Ministère de la santé et de l'action sociale, Direction général de la santé
1
Direction de Lutte contre la Maladie, Ministère de la Santé Publique, RD du Congo
1
Direction de Lutte contre la Maladie, Ministère de la Santé Publique, République Démocratique du Congo
1
Direction des Pharmacies et du Médicament
1
Direction du Développement et de la Coopération DDC
1
Direction general de estadistica, encuestas y censos, Paraguay et al.
1
Directorate General of Drug Administration,, Ministry of Health and Family Welfare, People's Republic of Bangladesh
1
Directorate General of Health Services
1
Directorate General of Health Services Ministry of Health & Family Welfare Government of the People’s Republic of Bangladesh
1
Directorate of Nursing Services
1
Directorate of Public Health and the Mycobacteria Group
1
Direito é Qualidade
1
Disability Inclusive and Accessible Urban Development (DIAUD)
1
Disability Rights Promotion International
1
Disability Studies Quarterly
1
Disability, CBR & Inclusive Development Journal (DCIDJ)
1
Disabled People South Africa (DPSA)
1
Division of International Protection
1
Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Coordinating Center for Health Promotion, Centers for Disease Control and Prevention, Department of Health and Human Services,
1
Divisions of Community Health Services, UNICEF
1
Dixius, A.
1
Dlouhy, M.
1
DNDi - Drugs for neglected diseases initiative
1
Do M, Hotchkiss D
1
Doeffinger, T.
1
Doherty, Meghan
1
Dolan CB, Saunders M, BenYishay A
1
Don Gorman and Wendy Cross
1
Donald A Enarson, Susan M Kennedy, David L Miller
1
Donald Dickerson and Aliyu Aminu Ahmed
1
Donald S Persons
1
Donaldson, Liam
1
Donatien Beguy 1 , Joyce Mumah , Salome Wawire , Kanyiva Muindi 1, Lindsey Gottschalk and Caroline W. Kabiru
1
Donkor, Peter
1
Donnelly, S
1
DOTS, WHO
1
Doubova SV, Leslie HH, Kruk ME, et al.
1
Douglass, Janet
1
Dove Medical Press Limited
1
Dovepress
1
Dovepress open access to scientific and medical research
1
Dowse, R.
1
Doyle, M.P.
1
DR
1
Dr Brink A. J., MD A P Messina, BPharm Prof C. Feldman, et al.
1
Dr F Siyoi, Dr C Forshaw, Dr J Mbuva ,Dr M Thuo, Dr N Mucheru, Dr E Ominde-Ogaja, Dr R Mbindyo, Mrs R Kirika
1
Dr Giraud Ekanmian
1
Dr Habib Ganfon
1
Dr Jean-François Trani and Dr Betsy VanLeit
1
Dr Nancy Baron
1
Dr T Apalata, Dr C Bamford, Mr D Benjamin et al.
1
Dr. Bin Bishr, A
1
Dr. A. Kumar
1
Dr. A. M. Z. Hussain
1
Dr. I. Chikovani
1
Dr. J. M. Caldas de Almeida
1
Dr. J. Rule
1
Dr. Janardhan N Navaneetham, Shravya Raghunandan, D M Naidu, H Hampanna
1
Dr. Joseph Sitienei OGW
1
Dr. K. Asiedu
1
Dr. Luis Távara Orozco
1
Dr. M. Dara
1
Dr. Md. A. Hasan
1
Dr. med. A. Aweimer
1
Dr. med. K. Behrendt
1
Dr. N. Shengelia
1
Dr. Qavi
1
Dr. R. Mahmud et al.
1
Dr. R. S. Gupta
1
Dr. Raviglione, M.
1
Dr. Rizvi
1
Dr. S. A. J. Md. Musa
1
Dr. S. Eyangoh et. al.
1
Dr. Sabita Malla (The Micronutrient Initiative (MI), Ministry of Health Nepal)
1
Dr. Scherpbier, R.
1
Dr. Supik, L.
1
Dr. T. Waite
1
Dr. T. Plümecke
1
Dr. Tulio Núñez Medina, et al.
1
Dr. V. A. Basauri
1
Dr. Vernet G
1
Dr. Will, A.
1
Dr. X. Zeka
1
Dr. Стивена Грэхема, Dr. Малгосии Грземска, Dr. Сюзанны Хилл et al.
1
Dr.H.Susilo Bambang Yudhoyono, President of the Republic of Indonesia
1
Dra. María Cristina San Miguel de Vera
1
Dreher, A.
1
Dressler D. D., MD, MSc Director OF
1
Driscoll, A.J.
1
Drs. Juan P. González-Rivas, Franmar Castellanos Barrios, Mariflor Vera, et al.
1
Drs. Marinela Falcone, Vicente Finizola-Flores
1
Druetz T.
1
Drug Safety
1
Drug Safety Monitoring Programme
1
Drugs Advisory Board, Republic of Botswana (Gabarone, Botswana)
1
Drugs for Neglected Diseases initiative DNDi
1
drugs.com
1
DSD, DWCPD and UNICEF
1
Du Plessis, A.L.
1
Duarsa, G.W.K., D.M. Soebadi, A. Taher, et al.,
1
Dube, A.
1
Duffy, M.
1
Duke UniversityMedical Center, Durham
1
Dunbar, E.L. et al.
1
Dunkel, J.
1
Durable Peace Programme Consortium
1
Durão, S.
1
Durrheim, D.
1
Dutch Association of Abortion Specialists (NGvA)
1
Dutra, W.
1
Dutta, S.
1
Dwyer, S.C.
1
Dyar O.J., B. Beovic, C. Pulcini et al.
1
Dzabala, N. et al.
1
E Clinical Medecine (Published by the Lancet)
1
E de Bruijn, M.
1
e National Institute of Statistics of Rwanda (NISR), the African Institute for Development Policy (AFIDEP) and UNFPA
1
E van‘t Hof, P Cuijpers, W Waheed, DJ Stein
1
E. A. Cooreman
1
E. Alarcón, C. Figuero, et al.
1
E. André
1
E. B. Pérez
1
E. B. Pérez
1
E. Baron, E. Breuer, et al.
1
E. Barrios Kuck
1
E. Bui
1
E. Castro-Costa, et al.
1
E. Chiappini
1
E. Corbett
1
E. Garralda, et al.
1
E. Geng
1
E. Gjergji
1
E. Goldson, Z. Abubakar et al.
1
E. Heseltine
1
E. J. Abrams
1
E. Jané-Llopis
1
E. L. Petroski
1
E. Levy Yeyati
1
E. M. Pitsoane
1
E. Masaki
1
E. McCloskey
1
E. O. Ekundayo, O. Onuka, G. Mustapha, et al.
1
E. Okitolonda
1
E. Pavlenko, A. Barbova, A. Hovhannesyan, et al.
1
E. Puca
1
E. Ross
1
E. Ruadze
1
E. Serván-Mori
1
E. Subata,
1
E. Tambo
1
E. Toska, et al.
1
E. Venturini
1
E. Vieta, T. Ahmed Okasha, et al.
1
E. VII Mballa Elanga
1
E. Villalobos Prats, A. Sena et al.
1
E. Zhou
1
E.-M. Berens, Klinger, J.
1
E.A Akl, S. Duda, et al.
1
E.A. Espinoza Fiallos, J.O. Robles Ticas
1
E.G. Brown Jr, D.S. Dooley, K. Smith
1
E.J. Rakotonirina, L.A. Raharitiana, L. Ravaoariso, et al.
1
E.M. Févre
1
E.Schuler
1
E.Z Asbu, O. Walker and J. M Kirigia, et al.
1
EACS (European AIDS Clinical Society)
1
EACS European AIDS Clinical Society (Европейского клинического общества СПИДа)
1
EAGA
1
ealth and Living Conditions Network of the European Observatory
1
East African Medical Journal
1
East and Central African Journal of Surgery
1
EAT Lancet Commission
1
Eaton, Jeffrey W.
1
Eba, B.
1
Ebehard, F.
1
Ebens, B., E. Fosse, M. Niechzial, et al.
1
Ebola Anthropology Platform
1
Ebuenyi, I.D.
1
Echazarreta, A.
1
Echeverry, M. C.
1
ECHO
1
Eckstein, D.
1
Economic and Political Weekly
1
Economic Commission for Latin America and the Caribbean (ECLAC),
1
EcoSan Club
1
Ecuador, Ministerio de Salud Pública
1
EDC (Education Development Center)
1
Edgar Carrasco, Enrique González
1
Edições UNESCO (Organização das Nações Unidas para a Educação, a Ciência e a Cultura)
1
Edielu, A.
1
Education Development Center
1
Education International
1
Education Santé
1
EducaVison Inc.
1
Egan, F.K.
1
Eglantina Dervishi
1
ehra (eurasian harm reduction association)
1
Eiling, E. & van Diggele-Holtland, M.
1
Einstein Journal
1
Ejembi, Clara Ladi, Tukur Dahiru, and Alhaji A. Aliyu
1
EKD
1
El Arnaout, N., Rutherford, S., Zreik,, et al.
1
El Gobierno des Todos, Ecuador
1
Elaine Abrams, Wafaa El-Sadr, and Miriam Rabkin
1
Elfriede-Dietrich-Stiftung hat die Deutsche Gesellschaft für Psychotraumatologie (DeGPT)
1
eLife
1
eLife Sciences Publications
1
Elisabeth Pitts
1
Elizabeth Glaser Pediatric AIDS Foundation
1
Elizabeth Glaser Pediatric AIDS Foundation
1
Elizabeth Glaser Pediatric New Horizons (Advancing Pediatric HIV Care)
1
Elke Müllegger, Günter Langergraber, and Markus Lechner
1
Elphick, J., De SasKropiwnicki, Z. &Elphick, R.
1
ELRHA
1
Elsevier B.V.
1
Elsevier Editora Ltda.
1
Elvis E. Tarkang, Prosper M. Lutala
1
EMA European Medicines Agency
1
Emanuel, E.J., et al.
1
Emelurumonye I. N., A. Miglietta
1
Emergency Capacity Building Project
1
Emergency Medical Services Authority (EMSA) California
1
Emergency Medical Services for Children
1
Emergency Nutrition Network ENN
1
Emergency Operations and Emergency Response Team
1
Emma Mbalame
1
Emmanuel J. Kandusi
1
Emmanuel O. Irek, Adewale A. Amupitan, Temitope O. Obadare, Aaron O. Aboderin
1
Emmanuelle Buache & Sarah Roesli (Formation Bachelor)
1
EMSC
1
Encontros Bibli
1
ENCOVI, et al.
1
Encyclopedia on Early Childhood Development
1
END TBc1
1
Endress P.
1
Enfermedades Infecciosas y Microbiología Clínica
1
Engagement Global
1
Engelman, D. et al.
1
Engender Health
1
EngenderHealt;
1
EngenderHealth/
1
Environment and Society Programme
1
Environment International
1
Environment Systems & Decisions
1
Environmental Research Letters
1
Environmental Science and Pollution Research
1
Eperon, G.
1
Epidemic Surveillance and Response
1
Epidemic Surveillance Response (Rwanda)
1
Epidemiologisches Bulletin
1
Epilepsia
1
Epilepsy Foundation of America
1
Erasmus, L., Poluta, M. & Weeks, R.
1
Eric Bui, Bonnie Ohye, Sophie Palitz, Bertrand Olliac, Nelly Goutaudier, Jean-Philippe Raynaud, Kossi B Kounou & Frederick J Stoddard Jr
1
Eric Maskin, Célestin Monga, Josselin Thuilliez and others
1
Erika Duffell, Igor Toskin
1
Erika Sutter, Allen Foster and Victoria Francis
1
Eriksen, M.
1
Eriksen, Tor Erik
1
Erikson, Abigail
1
Erin Berry-Bibee, Melissa Chen, Kathryn Curtis et al.
1
ERJ Open Research
1
ERJ Open Research, part of the European Respiratory Society (ERS)
1
Erle C. Ellis
1
Ernst Klett Verlag
1
Erwinanto, A. Santoso, J. N. E. Putranto, et al.,
1
Erziehungsdirektion Kanton Bern, Amt für Kindergarten, Volksschule und Beratung (AKVB)
1
Escritório Regional da OMS para a África
1
ESDC
1
Eskay M., Onu V. C., Igbo J. N., Obiyo N., Ugwuanyi L
1
Eskender Eshetu Ali
1
Eskild Petersen , Mary E. Wilson , Sok Touch , Brian McCloskey , Peter Mwaba , Matthew Bates , Osman Dar , Frank Mattes , Mike Kidd , Giuseppe Ippolito , Esam I. Azhar , Alimuddin Zumla
1
Espira, L. M.
1
Essack S.Y., A.T. Desta, R.E. Abotsi et al.
1
Esterhuizen, J.
1
ESTHER Ensemble pour une Solidarité Thérapeutique Hospitalière En Réseaux
1
et al. (Джеймса Баера
1
et al.)
1
et al.,
1
et K. McDonald
1
et Ondoua Biwole V.
1
et.
1
et. al
1
et.al
1
etc al.
1
Ethioian Health Insurance Agency
1
Ethiopia, Ministry of Health
1
Ethiopian Health and Nutrition Research Institute Public Health Emergency Management Centre
1
Ethiopian Health and Nutrition Research Institute, Federal Democratic Republic of Ethiopia
1
Ethiopian Journal of Health Development
1
Ethnopharmacologia
1
Etienne V Langlois, Andrew Mc Kenzie, Helen Schneider & Jeffrey W Mecaskey
1
Eurohealth
1
EuroHealth Observer
1
Europe PMC Funders Group
1
European & Developing Countries Clinical Trials Partnership EDCTTP
1
European Academies Science Advisory Council
1
European AIDS Clinical Society (EACS)
1
European AIDS Treatment Group
1
European Association for the Study of the Liver
1
European Centre for Disases Prevention and Control ECDC
1
European Coalition for Community Living
1
European Commission Directorate-General for Health and Food Safety
1
European Commission EC
1
European Commission, Directorate-General for Health and Consumers (DG SANCO)
1
European Commission, Humanitarian Aid
1
European Commission’s Humanitarian Aid and Civil Protection department (ECHO) and Oxfam
1
European Council on Refugees and Exiles (ECRE), Asylum Information Database (AIDA)
1
European Heart Journal
1
European Medicine Agency
1
European Medicines Agency EMA
1
European Migration Network
1
European Network for Diagnostics of Imported Viral Diseases
1
European Neurology
1
European Observatory on Health Systems and Policies Eurostation
1
European of Psychotraumatology
1
European Public Health Alliance
1
European Public Health Alliance (EPHA), Changing Markets
1
European Public Health Association
1
European Respiratory Journal (ERJ)
1
European Respiratory Journal, part of the European Respiratory Society (ERS)
1
European Respiratory Society
1
European Resuscitation Council
1
European Resuscitation Council ERC
1
European Society for Child and Adolescent Psychiatry ESCAP
1
European Society of Clinical Microbiology and Infectious Diseases EUCAST
1
European specialist nurse organisation (ESN)
1
European Union (EU)
1
European Union Agency for Fundamental Rights
1
European Union Civil protection and Humanitarian Aid
1
European University Institute
1
Eurosurveillance
1
Eurosurveillance (Europe’s journal on infectious disease epidemiology, prevention and control)
1
EVA JACQUELINE ETONGUE MAYER
1
Eva Jacqueline Etongué Mayer
1
Eva-Svoboda
1
Evangelia Kampouri, Shyma Jundi, Nida Sheriff et al.
1
Evangelina IN, Inês T, Miguelhete L et al
1
Evans, J.
1
Evelina Tacconelli, Michael Buhl, Hilary Humphreys et al.
1
Evert, J.
1
Evidence to Action
1
Ewig S.
1
Expert Committee on Pediatric Epilepsy, Indian Academy of Pediatrics
1
Expert Group on Disability
1
EXPERT REVIEW OF ANTICANCER THERAPY2020, VOL. 20, NO. 4, 271–278
1
Extending Service Delivery (ESD) Project, USAID
1
Eyring V., Gillett N. P., et al.
1
Ezea, CO.
1
Ezewudo, BI.
1
F. A. E. Sosso, O. Nakamura
1
F. Anam
1
F. Ayala
1
F. B. Assumpção, Jr
1
F. Bajunirwe
1
F. Becerra
1
F. Biadglegne, U. Sack, A. C. Rodloff
1
F. Bozzani et al.
1
F. Braddick
1
F. D.Zepf
1
F. Dibari and M. Myatt
1
F. Dockhorn Costa Johansen
1
F. Federspiel
1
F. Fezeu
1
F. Filippini
1
F. Gebissa
1
F. Griffiths, and J. Goudge
1
F. Kayambo
1
F. Kiweewa, A.Dasgupta
1
F. Lambert
1
F. M. Arenas, P. Loock
1
F. Ndugulile
1
F. Njenga
1
F. Norström, M. Y. Bertram et al.
1
F. O. Fasina, Fasanmi O.G., Makonnen Y. J., et al.
1
F. Odhiambo
1
F. Portaels
1
F. S.Sarfo, M. Sarpong Duah, et al.
1
F. Samuels
1
F. ScazzusoII
1
F. Tafese
1
F. Tavaglione
1
F. Terris-Prestholt
1
F. Tumwebaze
1
F. Verde
1
F. Zerbinato Bispo Velasco, de Oliveira Pedroza, G.G. et al.
1
F. Zermoglio
1
F.A. Prasetyo
1
F.Simona,E.Javellea ,A.Cabie, et al.
1
F1000 Research
1
F1000Research
1
Fabienne Heiniger
1
Facts Standard of Care for HIV and Coinfections in Europe
1
Faculté de Droit et de Science politique
1
Faculté de Médecine, Université de Sherbrooke
1
Faculty of Health Sciences, University of Pretoria South Africa
1
Fadahunsi, W.
1
Fahal, A.
1
Fairhead, J.
1
Fairlamb, A.H.
1
Fairlie, L.
1
Faiz, M.
1
Fajolu, I.
1
Falkenmark, M.
1
Fall, C. et al.
1
Family Planning Section
1
Fanning, A.
1
FAO
1
Farina A.
1
Farrukh, L.
1
Fassin D.
1
Fast SM, Mekaru S, Brownstein JS, Postlethwaite TA, Markuzon N.
1
Fast-Track Cities
1
FAU
1
Fauci AS, Morens DM
1
Fauziah, N.
1
Fay, K.A. et al.
1
Faye S. L., J. L. Ndiaye, S. Ba et. al.
1
Fazzone M.
1
Feasey, H. R. A.
1
Federación Internacional de Sociedades de la Cruz Roja y Media Luna Roja
1
Federal Bureau of Prisons
1
Federal Democratic Republic of Ethiopia Ministry of Health
1
Federal Democratic Republic of Ethiopia, Ministry of Health
1
Federal Government of Nigeria
1
Federal Ministry of Health
1
Federal Ministry of Health (FMOH), National Health Insurance Scheme (NHIS) and the National Primary Health Care Development Agency (NPHCDA)
1
Federal Ministry Of Health - Nigeria Centre for Disease Control
1
Federal Ministry of Health Nigeria , World Health Organisation (WHO)
1
Federal Ministry of Health of Ethiopia
1
Federal Ministry of Health, Ethiopia
1
Federici, M.
1
Federschmidt, K.
1
Feed the Future
1
Feinstein International Center, Tufts University
1
Fene, F.
1
Feng,S.
1
Ference, B.A.
1
Ferguson, S.
1
Fernanda Zermogli, MacKenzie Dove
1
Fernandes Maia, C.M.
1
Fernando R.
1
Ferrante, G.
1
Ferreira, J.P.
1
Ferreras, E.
1
Ferres M., Potin M.
1
Ferreyra C., D. O’Brien, B. Alonso
1
Ferri
1
Ferrin, M.
1
Fescina R, De Mucio B, Ortíz El, Jarkin D.
1
Feune de Colombi, N.
1
Fewer S.
1
Fédération internationale des Sociétés de la Croix - Rouge et du Croissant - Rouge
1
fhi 360
1
Field Epidemiology Services (Public Health England)
1
FIGO Committee for Women’s Sexual and R eproductive Rights
1
FIGO et partenaires
1
FIGO LOGIC
1
Figueiredo, C. A.
1
finep, forum für internationale entwicklung + planung
1
Fiona Charlson, Suhailah Ali, Jura Augustinavicius et al.
1
Fiona Gell, Eliza Hilton, Tess Dico-Young
1
FIP Working Group on Pharmacists and HIV-AIDS
1
Firdaus, I., A.U. Rahajoe, A. F. Yahya, et al.,
1
Firth, J. et al.
1
Fishel, Joy D., Ruilin Ren, Bernard Barrère, and Trevor N. Croft
1
Fistuale Care
1
Fitzgerald, D. A.
1
Fitzgerald, D.A. et al.
1
Fitzgerald, F.
1
Flatten, G., Gast, U., Hofmann, A., Knaevelsrud, C., Lampe, A., Lieberman, P., Maercker, A., Reddemann, L. & Wöller, W.
1
Flaurine J - J. Joseph et al.
1
Flor, L.S.
1
Florey, Lia
1
Florian Daniel Zepf, Caroline Sarah Biskup, Martin Holtmann, &
1
Florian Lederbogen, Leila Haddad, Andreas Meyer-Lindenberg
1
Florida International University
1
Flory A. et al.
1
Flory, L.
1
Flueckiger, P.
1
Flüchtlingshilfe München e.V.
1
Flying Publisher
1
Flying Publisher, Boehringer Ingelheim
1
FOCUS
1
Folb, N., Levitt, N.S., Backmann, M.O., et al
1
Fondo de las Naciones Unidas para la Infancia (Unicef)
1
Fondo de Población de las Naciones Unidas
1
Fonds Africain de Développement
1
Fonds des Nations Unies pour la population
1
Fongwen, N.
1
Fontaine, Julie
1
Food and Agriculture Organization of the United Nations (FAO)
1
Food and Agriculture Organization of the United Nations FAO and World Health Organization WHO
1
Food and Agriculture Organization of the United Nations FAO, World Health Organization WHO
1
Food and Agriculture Organization of the United Nations FAO, World Health Organization WHO and World Organisation for Animal Health OiE
1
Food and Agriculture Organization on the United Nations
1
Food and Drug Administration (FDA)
1
Food and Nutrition Technical Assistance II Project (FANTA - 2)
1
Fooks, A.
1
Forbes J.
1
Foreign Affairs, Trade and Development Canada
1
Formation VIH
1
Forsberg, B.
1
Forum of International Respiratory Societies
1
Forum on Neuroscience and Nervous System Disorders
1
FosterA.
1
Foundation for innovative new diagnostics FIND
1
Founou, L.L.
1
FP2020 - Avenir Health
1
Frahm, I. L.
1
Frances Javier, Julie Chilton & Andrés Martin
1
Francis Aboagye-Nyame, Heather Alexander, Zelalem Gizachew Belachew et al.
1
Franckling-Smith, Z.
1
Franco J, Simarro P, Diarra A, Jannin J
1
Franco Mascayano, Thamara Tapia, Sara Schilling, Rubén Alvarado, Eric Tapia, Walter Lips, Lawrence H. Yang
1
Franco, JR.
1
Frank Shann and John Vince
1
Frank, A.
1
Frank, Ti.
1
Frase N. S.
1
Fraser V, Hunt MR, Schwartz L, and de Laat S
1
Frauenhauskoordinierung e.V. (FHK)
1
Frean J., Sieling W., Pahad H. et al
1
Frederic Mousseau
1
Fredrick K. Sawe
1
Freedman, B.
1
Freeman, M.C.
1
Frempong, K.K.
1
Frewer, A.
1
Frédéric Kobelembi, F.
1
Friedman, J.F. et al.
1
Friedrich-Ebert-Stiftung
1
Friedrich-Ebert-Stiftung (FES)
1
Friel, S.
1
Frimpong, M.
1
Fritsch, P.
1
Fritsche, A.
1
Front. Public Health
1
Frontiers in Chemistry
1
Frontiers in Immunology
1
Frontiers in Reproductive Health, Family Health Department, Ministry of Health and Social Welfare, Kingdom of Lesotho
1
Frontiers in Veterinary Science
1
Fröber,J.
1
Fuchs A., J. Bielickia, S. Mathur, et.al.
1
Fuchs, A. and Öhler, H.
1
Fuentes J, Bakare M, Munir K et al.
1
Fuentes-Alabi S.
1
Fuller, R.
1
Fundación Celestina Pérez de Almada, et al.
1
Fundación Seguros Caracas
1
Fundação Calouste Gulbenkian
1
Fundo de População das Nações Unidas
1
Fung
1
Fuss, A.
1
Fuster, V.
1
Futures
1
G, Zambrano, E Salgato, F. M. Moyano et al.
1
G. Abiyu, et al.
1
G. Ayala, J. Garay, M. Aragon, et al.
1
G. B Kulkarni
1
G. B. Migliori, E. Pontali, G. Sotgiu, et al.
1
G. Bartlett
1
G. Behrens
1
G. Bishwajit, C. Zhaohui, H. Zhifei
1
G. Divan
1
G. F. Tchouwa
1
G. Franco-Sotomayor
1
G. Gogia
1
G. Greco et al.
1
G. Gururaj
1
G. H. Loneragan, H. M. Scott et al.
1
G. H. Mazurek, J. Jereb, P. LoBue et. al
1
G. Hirnschall
1
G. J. Montalto
1
G. J. Weil
1
G. Jonsson
1
G. Kyselyova
1
G. L. Birbeck
1
G. Lende
1
G. Lescornec
1
G. M. Kassa
1
G. M. Montes Zuluaga, F.N. Alcalde-Rabanal et al
1
G. McCord
1
G. N. Rao
1
G. Ooms
1
G. O’Hara
1
G. Rogers
1
G. Rundgren and N. el-Hage Scialabba
1
G. S. Bel
1
G. Sander, A. Scandurra, A. Kamenska, et al.
1
G. Sander, R. Lines
1
G. van Cutsem
1
G.A.Williams, G. Scarpetti, et al.
1
G.C Frey, and V. A Temple
1
G.H. Wills, E. Wobudeya, et al.
1
G.Reith, E. Langham, et al.
1
G.S. Wallace& J.F. Seward
1
G4Alliance for surgery, obstetric, trauma and anesthesia care
1
Gabriel Coulibaly, Astrid Meyer et Sabine Dorlöchter-Sulser
1
Gabrys, J.
1
Gabrysch, Sabine
1
Gadea, P.
1
Gaël D. Maganga, D.V.M., Jimmy Kapetshi, Nicolas Berthet, et al.
1
Gage A., Leslie H., Bitton A., et al.
1
GAIN & Johns Hopkins University
1
Gajda M., E. Urban
1
Galarraga, O.
1
Galarza, P. et al.
1
Gallo-Bernal, S.
1
Gallup
1
Gamez, Laura et al.
1
Gandaho T., C. Striefel, M. Maiga et. al.
1
Gaona Narváez, J.
1
Garcia C., Abreu L., Ramos J. , et al.
1
García, J.M.
1
García-Mostajo, J.A.
1
Gardin B.
1
GARDP Global Acntibiotic Research & Dedvelopment Partnership
1
Garratt, A.
1
Garrison Institute
1
Gary N. Siperstein, Ph. D. Keerthi Sugumaran, Jennifer Norins Bardon, Robin C. Parker, M.S. University of Massachusetts Boston
1
Gascon M., Markevych I.
1
Gastroenterology Society of Kenya , Republic of Keny
1
Gatzweiler F., Lindgren E., et al.
1
Gauri Divan
1
GAVI Alliance
1
GAVI The Vaccine Alliance
1
Gavilanez Medina Patricia, Gualoto Lincango Blanca, Chamorro Obando Patricia et al
1
Gawande, Atul
1
Gayenell S. Magwood, Michelle Nichols et al
1
Gaziano, T. et al.
1
Gaziano, Thomas A.
1
GBD 2019 Blindness and Vision Impairment Collaborator
1
GBD 2019 Blindness and Vision Impairment Collaborators
1
GBD 2019 Ethiopia Subnational-Level Disease Burden Initiative Collaborators
1
GBD 2019 Human Resources for Health Collaborators
1
GBD 2019 Tuberculosis Collaborators
1
GBD2019 Dementia Forecasting Coolaborators
1
GBI
1
Gebreselassie, Tesfayi, and Pav Govindasamy
1
Geissler, C.
1
Gelband, Hellen
1
Geldsetzer, P.
1
Generalitat de Catalunya Department de Salud
1
Geneva Global Health Hub
1
Geneva International Centre for Humanitarian Demining (GICHD)
1
GeoPoll
1
George, G., Atujuna, M. & Gow, J.
1
Georgette Mulheir
1
Georgios Nikolopoulos, University of Cyprus
1
Gerald Keusch, Keith McAdam, Patricia Cuff, Michelle Mancher, and Emily R. Busta
1
Gerald L. Klerman, Myrna M. Weissman et al.
1
Geraldine Le Cuziat, Geraldine
1
German Bishops' Conference Research Group on International Church Affairs
1
German Diabetes Association (DDG)
1
German Federal Ministry for Economic Cooperation and Development (BMZ)
1
German Gymnastics Federation (Deutscher Turner-Bund, DTB)
1
German Institute for Medical Mission
1
German Resuscitation Council
1
Germanavicius, A.
1
Germano MP, Elena F, Ndlovu N et al
1
Germanwatch e.V.
1
Germany’s National Public Health Institute (RKI), et al.
1
Gertler, P. & Vermeersch, C.
1
GFATM
1
Ghana Statistical Service Ghana Health Service Accra, Ghana
1
Ghanaian Parliament
1
Ghosh, A.
1
GHS/NMCP/JHPIEGO/MSH/GLOBAL FUND (GFATM)
1
Gibson, A.
1
Gideon
1
Gil, A.
1
Gilbert, B.J.
1
Gildas Agodokpessi, Nadia Aït-Khaled, Martin Gninafon, Leon Tawo, Wilfried Bekou, Christophe Perrin, Karen Bissell, Nils Billo, Donald A Enarson, Chen-Yuan Chiang
1
Gillini, L.
1
Gilma Mantilla
1
Gilman, R.T.
1
Gilson, R.
1
Giordani, F.
1
Giorgio Guzzetta, Fabrizio Montarsi, Frédéric Alexandre Baldacchino et al.
1
Giovanny Vinícius Araújo de França, Valdelaine Etelvina Miranda de Araújo et al.
1
Gjergji, M.
1
Gleeson, T.
1
Glenn, B. E.
1
Global Antibiotic Resistance Partnership—Tanzania Working Group
1
Global Tuberculosis Proqramme, World Health Organization
1
Global Alliance for Improved Nutrition gain (GAIN)
1
Global Alliance for Vaccines and Immunisation (Gavi)
1
Global Asthma Network
1
Global Centre for the Responsibility to Protect
1
Global Clubfoot Initiative (GCI)
1
Global Coalition for Circulatory Health
1
Global Commission on Drug Policy
1
Global Dynamics of Social Policy
1
Global Forum on MSM & HIV
1
Global Fund, World Bank Group, Gavi, the Vaccine Alliance et al.
1
Global Handwashing Day
1
Global Healp
1
Global Health & Medicine
1
Global Health Alliance-Deutschland (GHA-D)
1
Global Health Cluster
1
Global Health Workforce Alliance
1
Global Initiative on Psychiatry (GIP)
1
Global Institute for Asthma
1
Global Journal of Human-Social Science
1
Global Laboratory Initiative (GLI), Stop TB Partnership
1
Global mental health (Atilola, O.)
1
Global mental health, Cambridge University Press
1
Global Network for Neglected Tropical Diseases
1
Global Network of People Living with HIV (GNP+), International Community of Women Living with HIV (ICW) et al.
1
Global Nutrition Cluster
1
Global Nutrition Report Stakeholder Group
1
Global Partners in Care
1
Global Polio Eradication Initiative
1
Global Preparedness Monitoring Board
1
Global Protection Cluster, GPV Prevention and Response
1
Global Research on Developmental Disabilities Collaborators
1
Global smart
1
Global Social Service Workforce Alliance, UNICEF
1
Global Task Force for Cholera Control
1
Global Task Force on Cholera
1
Globalisation and Health Initiative (GandHI).
1
GMDAC, University of Potsdam
1
GNP (Global Network of people living HIV)
1
GNP+ (Global Network of people living with HIV)
1
GOARN
1
Gobierno Bolivariano de Venezuela, UNICEF, et al.
1
Gobierno de Cantabria
1
Gobierno de la Republica Guatemala
1
Godard, P.
1
Godfrey, E.
1
Goff, D.
1
Goh, N. S. L.
1
Gojka Roglic, Cherian Varghese, Leanne Riley et al.
1
Golledge, J.
1
Gollob, K.
1
Gomes Machado, F.C. et al.
1
Gonzales N., et al.
1
González Sanjuan, S.
1
Gordon, C.
1
Gottlieb N., N. Davidovitch, D. F. Filc et al.
1
Gottlieb, N., M. Hintermeier, K. Bozorgmehr
1
Gould, M.K.
1
GOV.UK developer docs
1
Govender, K.
1
Governance and Social Development Resource Centre
1
Governance and Social Development Resource Centre HEART
1
Governement of Nepal, Family Health Division Department of Health Services
1
Government Gazette
1
Government of Bangladesh
1
Government of Ethiopia
1
Government of Ghana
1
Government of India
1
Government of India, National Disaster Management Authority
1
Government of Japan, World Bank, GFDRR
1
Government of Nepal Ministry of Health Department of Health Services Leprosy Control Division
1
Government of Nepal Ministry of Education Department of Education
1
Government of Nepal Ministry of Health and Population Curative Services Division
1
Government of Nepal Ministry of Health and Population Department of Health Services
1
Government of Nepal Ministry of Health and Population Department of Health Services, National Centre for AIDS and STD Control
1
Government of Nepal, National Planning Commission
1
Government of Nepal, UN Educational, Scientific and Cultural Organization
1
Government of Nepal, Ministry of Health and Population, National Centre for AIDS and STD Control
1
Government of Nepal, National Planning Commission (NPC)
1
Government of Nepal, National Planning Commission, Secretariat Central Bureau of Statistics, The World Bank
1
Government of Nepal,Ministry of Health and Population, Department of Health Services
1
GOVERNMENT OF SIERRA LEONE MINISTRY OF HEALTH AND SANITATION
1
Government of Sierra Leone, Department for International Development, UN Population Fund, Irish Aid
1
Government of SomaliaWorld Health Organization WHO
1
Government of South Africa
1
Government of Southern Sudan, Ministry of Health
1
Government of the Democratic Republic of the Congo, World Health Organization
1
Government of the Federal Democratic Republic of Ethiopia
1
Government of the People's Republic of Bangladesh
1
Government of the Philippines
1
Government of the Republic of Namibia
1
Government of the Republic of South Africa
1
Government of Timor-Leste
1
Government of Zimbabwe
1
Governo de Estato Sao Paulo
1
Governo Federal Brasil
1
Governo Federal Brasil, Sistema Único de Saúde, Secretarias Estaduais e Municipais de Saúde, Ministério da Saúde Brasil
1
Gölz, S.
1
GP clinics
1
Grace A. K. Ettyang & Caroline J. Sawe
1
Grace Musoke & Priscille Geiser
1
Grace, D.
1
Grace, K.
1
Graf, J.
1
Graham H., Lampard P., et al.
1
Grampari
1
Grand’Maison P.
1
Graves B.N.
1
Graves C. et al.
1
Graves, Patricia
1
Gray, C.L.
1
Gray, Robin
1
Greaves, C.J.
1
Greco, G.
1
Green Ink
1
Green, C.
1
Green, R.J. et al.
1
Greenhalgh, T.
1
Greenstone, M.
1
Gregorowski, C. & Seedat, S.
1
Gregory H Cohen, Shailesh Tamrakar, Sarah Lowe, et al.
1
Greinacher, A., et al.
1
Grépin K.
1
Gribble RSF, Liese BH, Wickremsinhe MN
1
Grimshaw, J. M.
1
Grohol, J.
1
Grollman C.
1
Grote, J.
1
Grotenhuis, R.
1
Groupe de travail interorganisations sur la santé reproductive en situations de crise
1
Groupe spécial mondial de lutte contre le Choléra
1
Groupe URD
1
Growth Analysis Studentplan
1
Gruber, F.
1
Gruetzmacher, K.
1
Grupo de Entomologia, Instituto Nacional de Salud
1
GRUPO ESPECIAL MUNDIAL DE LUCHA CO NTRA EL CÓLERA
1
Gualtero Trujillo, S. M.
1
Gubbins, P.
1
Guimaraes, Alice Soares
1
Gulev S. K., Thorne P. W. et al.
1
Gulsuner, S. , D. J. Stein, E. S. Susser, et al.
1
Gunaratne, C., Kremer, P.J., Lewis, A.J. & Clarke, V.
1
Gunton R. M., Hejnowicz A.P.
1
Guo Y., , Ye T., et al.
1
Guo, J.
1
Gupta, A.
1
Gupta, R.
1
Gureje, O.
1
Gury S. et al.
1
Gustavo Corrêa, G.
1
Gutiéerrez, J.
1
Gutiérrez, J.
1
Gutson, K.
1
Guzman C., Potter T.
1
Guzman-Vilca, W. C.
1
Guzmán M.
1
Gwynnyth Llewellyn, Eric Emerson, Ros Madden and Anne Honey
1
Gyapong, J.
1
Gyssens I. C., W. V. Kern, D. M. Livermore
1
H. Adler, Gould, S.
1
H. Advani
1
H. B. Abdullah
1
H. Bailey et al.
1
H. Bergmann
1
H. E. Erskine
1
H. E. Hutton et al.
1
H. E. Jenkins, V. Crudu, V. Soltan, et al.
1
H. Flynn
1
H. Fuenzalida
1
H. Furtmayr, K. Krása
1
H. Garrison-Desany
1
H. H. Nguyen
1
H. Hafizi
1
H. Huerga
1
H. Korn
1
H. Kuper and K. Blanchett , et al.
1
H. Kurtis
1
H. L. Rieder, A. Van Deun, K. M. Kam, et. al
1
H. Petkova, A.D. Tsouros, et al.
1
H. Ronald
1
H. S. Faich Dini
1
H. Sakamoto
1
H. Schneider and T. Puoane
1
H. Sloot
1
H. Stutzman et al.
1
H. T. Ayele, M. S. M. van Mourik, T. P. A. Debray, et al.
1
H. Thirumurthy, E. Omanga, B. Obonyo et al.
1
H. Visser, de Bruin S., Knoop J. et al.
1
H. Visser, de Bruin S., Knoop J. , et al.
1
H. Wardle and I. Gilmore
1
H. Yeboah
1
H.d Sobel
1
H.D. Mazigo
1
H.Desta, T.Berhe and S. Hintsa
1
H.E. Drummer
1
H.J.G. de Kok
1
H.J.Kim
1
H.Kanyerere, A.D. Harries, K. Tayler-Smith, et al.
1
H.N.C. Yoder, W..Tol, R. Reis and J.T.V.M. deJong
1
Haab, G. A., et al.
1
Haak, T.
1
Haarmann, E.
1
Habeeb, K. et al.
1
Haddad L., Verburg G., Fore H., et al.
1
Haefele-Abah, C.
1
Haematologica
1
Hagan, J.
1
HAI
1
hai global
1
Haid Haid
1
Haider, N.
1
Haitham Shoman, Emilie Karafillakis and Salman Rawaf
1
Haja R. Wurie, Mohamed Samai and Sophie Witter, Human Resources for Health
1
HAL archives ouvertes
1
Halaharvi, H.
1
Hall, S.
1
Halloran A.
1
Halpin, E., Kugathasan, V., Hulbert, C., Alvarez-Jimenez, M. & Bendall, S
1
Hamid, H.
1
Hamilton I., Kennard H., McGushin A. et al.
1
Hamstead, Z.A.
1
Han, K.
1
Hana, S. et al.
1
Hanas, R.
1
Handicap International | Save the Children
1
Handley, B.
1
Hanigan, I. et al.
1
Hanlon C
1
Hanlon et al.
1
Hanlon, M.
1
Hannah Bowen
1
Hannah Faal, Rènée du Toit, Henrietta Monye, Ronnie Graham
1
Hannah Metzger, Sina Wanderer & Veit Roessner
1
Hanne M. Norseth1,2, Patricia D. Ndhlovu3, Elisabeth Kleppa, et al.
1
Hans L. Rieder, Armand Van Deun, Kai Man Kam, Sang Jae Kim, T. Martin Chonde, Arnaud Trébucq, Richard Urbanczik
1
Hansen, J.
1
Hantera, M.
1
Haq, Bashirul
1
Harald Lutz, and Elisabetta Buscarini
1
Harald T. Lutz Hassen A. Gharbi
1
Harborview Medical Center
1
Harding, J.L.
1
Harding, Kassandra L.
1
Harding-Zentrum für Risikokompetenz
1
Hariharan, N., Ishtiaq, A., Eldridge, C., et al.
1
Harinder Singh Chahal, Nazaire St. Fort, Lisa Bero
1
Harm Reduction Journal
1
Harmer, Adele
1
Harnmeijer J.
1
Harris. P.
1
Harrison Arroz, J
1
Harrison, J.A.K.
1
Harrison, V.
1
Hartley, S.
1
Hartman-Boyce J., N. Lindson
1
Harvard Humanitarian Initiative
1
Hasan Arshad, S.
1
Hasker E, Hope A, Bottieau E.
1
Hasman, A-
1
Hassan, G, Kirmayer, LJ, Mekki- Berrada A., et al.
1
Hassanein M., Afandi B. et al.
1
HAT & OND Team
1
Hategeka C, Carter SE, Chenge FM, et al.
1
Hatmann-Boyce J., N. Lindson
1
Haut Conseil de la Santé Publique
1
Haute Autorité de santé
1
Haute Conseil de la Santé Publique
1
Haute Ecole de la Santé la Source
1
Haver, Katherine
1
Hayley Gleeson
1
Haywood, A. and B. D Glass
1
Hazel Jones and Jane Wilbur
1
Hänselmann, A.
1
Håkon Angell Bolkan Donald Alpha Bash-Taqi Mohammed Samai Martin Gerdin Johan von Schreeb
1
HBSC
1
HDRC
1
Health Workforce Team of the World Health Organization Regional Office for Africa (WHO
1
HEALTH & FAMILY WELFARE DEPARTMENT GOVERNMENT OF ODISHA
1
Health Action International Africa
1
Health Affairs
1
Health and Education Advice and Resource Team
1
Health Care Analysis
1
Health Cluster
1
Health Cluster, WHO
1
Health Department: Republic of South Africa
1
Health Emergency Management Staff, DOH and WHO Philippines
1
Health Foundation
1
Health in Your Hands
1
Health Policy Project, Futures Group
1
Health Policy Project, USAID
1
Health Poverty Action
1
Health Professional Council of South Africa
1
Health Sector Support Program (HSSP)
1
Health Service and Population Research Department,Institute of Psychiatry, King's College London
1
Health Services Division of Ministry of Health and Family Welfare , Government of Bangladesh
1
Health Systems and Policy Research
1
Health Systems Trust
1
Healthcare Journal
1
Healthline
1
Healy, K.
1
Heart, BMJ journals
1
Hecker, T. & Maercker, A.
1
Heiligensetzer C.
1
Heiligensetzer, C.
1
Hejj, T.
1
Heleen van Beekhuizen and Regine Unkels
1
Helen Keller International
1
Helen Killaspy, Peter McPherson, Chiara Samele, Rene Keet, JM Caldas de Almeida
1
Helene Schwartz, ACF International Network
1
Heliyon
1
Hellen Gelband,Jha Prabhat, Rengaswamy Sankaranarayanan et al.
1
Help Age Internationl
1
HelpAge
1
HelpAge International Myanmar, University of Public Health and University of Medicine-2
1
Helping babies breathe
1
Helsinki Foundation for Human Rights, European Union
1
Helthcare Improvement Scotland
1
Henao-Restrepo, A.M.
1
Hendrik CJ van Rensburg
1
Henninger, B.
1
Henry B. Perry, Ranu S. Dhillon, Anne Liu, et al.
1
Hepatology Society of the Philippines
1
Hepatology Society of the Philippines (HSP)
1
Herazo, F.
1
Herdy, A.H.
1
Herman Woerdenbag
1
Hernández F.A.
1
Hernández, C. et al.
1
Herrera, G.
1
Hhary, EP.
1
Hickel, J.
1
Hidalgo, R.
1
Hijazi, Z.
1
Hill, A.
1
Hiller, R.M., Meiser-Stedman, R., Fearon, P., Lobo, S., McKinnon, A., Fraser, A. & Halligan, S.L.
1
Hillman
1
Hindawi Psychiatry Journal
1
Hindawi Publishing Corporation
1
Hindawi Publishing Corporation AIDS Research and Treatment
1
Hindricks, G.
1
Hine, P.
1
Hinnock, H.
1
HIP Family Planning High Impact Practices
1
Hitzeroth, J.
1
HIV
1
HIV and AIDS Ministry of Health
1
HIV Economics Reference Group
1
HIV i-Base
1
HIV i-BASE/TREATMENT ACTION GROUP
1
HIV law project
1
HIV Self-Testing Africa Initiative
1
HIV/AIDS - Research and Palliative Care
1
hivma
1
hler, Oliver Razum, Jean-Olivier Schmidt
1
Ho T., Cusack R.P., Chaudhary N. et al.
1
Hodge, M., Bolinas, A., Jaucian, E., et al.
1
Hodge, Matthew
1
Hoffman, S.
1
Hogg Foundation for Mental Health
1
Hogrefe Publishing
1
Hoines, K.
1
Holm, S
1
Holmes, King K.
1
Holt, E.
1
Holy See Press Office
1
Hommes F, Stratil J, Ströbele L, Bruchhausen W
1
Honein MA, Christie A, Rose DA, et al.
1
Hong‑Mei Luo
1
Hooiveld, M.
1
Hooman Ghrobani, Mahnoush Momeni, Ali Zavareh, Mahshid Aghajanzadeh, Maryam Roham, Hamid Karimi, Hossein Rahbar
1
Hopkins, D.
1
Hopper, J.
1
Hordern
1
Horn, D.
1
Hosny, H.
1
Hospice Palliative Care Association of SOUTH AFRICA
1
Hospital Divina Providencia
1
Hotez, P.
1
House, S.
1
Houston R, Acharya B, Poudel D, Pradhan S, Singh S, Manandhar M, Pokharel RK, Shrestha PR
1
Hoviyeh Afnan-Holmes, Moke Magoma, Theopista John, et al.
1
Howes, O.D.
1
Howse, E.
1
Hoy, R.
1
Hridaya Harm Reduction in India
1
hrp
1
HRSA
1
Hsia Y., B. R Lee, A. Versporten, et al
1
HSRSP, RTI International
1
Hsu J.
1
Hsu, J.
1
Hua Fu
1
Hua Yu
1
Huffman, M. et al.
1
Hugo Slim and Lorenzo Trombetta
1
Human Rights Watch and WASH (Water, Sanitation and Hygiene) United
1
Human Rights Watch HRW
1
Humanitarian Accountability Partnership (HAP)
1
Humanitarian Advisory Group
1
Humanitarian Disaster Institute
1
Humanitarian Evidence Programme, Oxford, Oxfam
1
Humanitarian Innovation Fund HIF
1
Humanitarian Practice Network (HPN)
1
Humanitarian Practice Network at ODI
1
Humboldt University Berlin, Research Programme on Religious Communities and sustainable developpment
1
Hunt, J.
1
Hunter, R.F.
1
Huque, S. et al.
1
Hurtado, J.J.
1
Hussain.H.
1
HVTB
1
Hwang, J.
1
Hynes W.
1
i-base
1
I. Bozicevic
1
I. Couto
1
I. Eramova
1
I. Faturiyele, D. Karletsos, K. Ntene-Sealiete, et al.
1
I. Feijo
1
I. Friesecke, W. Biederbick,G. Boecken, et al.
1
I. Fronteira
1
I. Frost
1
I. Gercama and J. Bedford
1
I. Hall
1
I. Henry
1
I. J. C. Schneider
1
I. Kirtadze
1
I. Kuznetsova, O.Mikheieva, J. Catling, et al.
1
I. Mbabali
1
I. Megiddo
1
I. Mokrousov, (St. Petersburg Pasteur Institute)
1
I. Oehler
1
I. Páez, D. Moreno et al.
1
I. Petersen
1
I. Sazonova
1
I. SECK
1
I. Semini
1
I. Steffens
1
I. T. Katz
1
I. Teplinskaya
1
I.J. Emodi
1
IACG Interagency Coordination Group on Antimicral Resistance
1
Ian R McClelland
1
IAPB Africa
1
IASC et al.
1
IASC Inter-Agency Standing Committee
1
IASS Potsdam
1
IATT
1
Ibarra-Cerdena, C.
1
ICAAP Secretariat
1
ICAP Columbia University
1
ICAP Nurse Capacity Initiative
1
ICAP, et al.
1
icco (Partner to enterprising people)
1
ICF International Calverton, Maryland, USA
1
ICMPD
1
ICRC - International Committee of the Red Cross
1
ICRW (International Center for Research on Women)
1
ICS
1
ICW Global
1
ICW Latina
1
ICW WA
1
Idika, IK.
1
Idro R, Musubire K A, Byamah Mutamba B
1
IDSA
1
IDSA, HIVMA, et al.
1
Iemmi, Valentina Gibson, Lorna Blanchet, Karl, et al.
1
IFRC - International Federation of Red Cross
1
IFRC, et al.
1
IFRC, UNICEF and WHO
1
IGAT Hope INC.
1
Igras, S., Sinai, I., Mukabatsinda, M., et al.
1
IGWG
1
Ihana Thaís Guerra de Oliveira Gondim
1
IHRD (International Harm Reduction Development)
1
ILGA-Europe (The European Region of the international Lesbian and Gay Association)
1
Illinois Institute of Technology
1
ILO International Labour Organization
1
Ilona Kickbusch
1
Ilona Kickbusch, Christian Franz, Anna Holzscheiter, Iris Hunger, Albrecht Jahn, Carsten Kö
1
ILRI
1
iMedPub
1
iMedPub Journals
1
iMMAP
1
IMPACT Initiatives UNHCR
1
Imperial College COVID-19 Response Team
1
Implementation Science
1
Ince, M.E. , R. Shaw and K. Davey
1
Inconnu
1
Independent Review Team
1
India HIV/AIDS Alliance
1
India State-Level Disease Burden Initiative CRD Collaborators
1
India State-Level Disease Burden Initiative CVD Collaborators
1
India State-Level Disease Burden Initiative Diabetes Collaborators
1
India State-Level Disease Burden Initiative Neurological Disorders Collaborators
1
India State-Level Disease Burden Initiative Suicide Collaborators
1
Indian Academy of Paediatrics
1
Indian Consensus of Medical Research
1
Indian Council of Medical Research & Department of Biotechnology
1
Indian Council of Medical Research (ICMR) & Department of Biotechnology
1
Indian Council of Medical Research (ICMR), Global Health Advocates, Cochrane Infectious Diseases Group
1
Indian Council of Medical Research - Department of Health Research
1
Indian Journal of Medical Ethics
1
Indian Journal of Psychiatry
1
Indian Pediatrics
1
Indian Society of Nephrology
1
Indonesian Drug Users Network
1
Indonesian Rheumatology Association
1
Indonesian Society of Endocrinology (ISE)
1
Indonesian Society of Internal Medicine
1
Infections & Morbidities
1
Infectious Diseases Society of America
1
Infectious Diseases Society of America (IDSA)
1
Informa Healthcare
1
INFORMED
1
Ingo Radtke
1
Ingrid Lewis and Sunit Bagree
1
Iniciativa ETMI-PLUS
1
Insfran J. D. M., Vicioso J. J. R. et al.
1
Institut de Formation et de Recherche Interdisciplinaires en sciences de la Santé et de l’Education (IFRISSE)
1
Institut de Médecine Tropicale, Université de Bordeau
1
Institut für Allgemeinmedizin Charité
1
Institut für Public Health und Pflegeforschung, Universität Bremen
1
Institut National de la Statistique (INSTAT) Madagascar et ORC Macro
1
Institut National des Recherches Agricoles du Bénin (INRAB)
1
Institute for Community Inclusion at University of Massachusetts
1
Institute for Community Inclusion UMass Boston
1
Institute for Public Policy Research
1
Institute for research in international assistance
1
Institute for Security Studies
1
Institute for Security Studies ISS
1
Institute of Development Studies, Aga Khan University
1
Institute of Economic and Social Research (INESOR), University of Zambia
1
Institute of Psychiatry
1
Institute of Public Health Nutrition (IPHN) et al
1
Institutional research information system iris
1
Institutional Treatment,Human Rights and CareAssessment (ITHACA)
1
Instituto de Estudios en Salud, Sexualidad y Desarrollo Humano (IESSDEH)
1
Instituto de Medicina Tropical, Paraguay
1
Instituto de Previsíon Social
1
Instituto Nacional de enfermedades respiratorias
1
Instituto Nacional de Salud Colombia
1
Instituto Nacional del Cancer and Ministerio de Salud, Argentina
1
Intebi, I.V.
1
Integration durch Sprache e.V.
1
Integritas
1
Inter Sector Coordination Group - Bangladesh
1
Inter-Agency Standing Commitee (IASC)
1
Inter-Agency Standing Committee (IASC) Reference Group for Mental Health and Psychosocial Support in Emergency Settings
1
Inter-Agency Task Team to Adress HIV in Humanitarian Emergencies
1
Inter-Parliamentary Union (For democracy, For everyone)
1
InterAction Council
1
Interagency Health and Nutrition Evaluations in Humanitarian Crises (IHE) Initiative
1
Interagency Policy Coordination Subcommitee for Preparedness & Response to Radiological and Nuclear Threats
1
Interagency Task Team HIV in Humanitarian Emergencies
1
interburns
1
Interdisciplinary Perspectives on Infectious Diseases
1
Internation Federation of Red Cross
1
International Agency for Prevention and Blindness
1
International AIDS Society (IAS)
1
International Alert
1
International Alert/ГІП-Тбілісі/Лондонською школою гігієни і тропічної медицини
1
International Association of National Public Health Institutes
1
International Bank for Reconstruction and Development
1
International Bank for Reconstruction and Development / The World Bank
1
International Centre for Diarrhoeal disease Research
1
International Centre for Evidence in Disability, London School of Hygiene & Tropical Medicine
1
International Centre for Eye Health
1
International Coll. Essential Surgery
1
International Comitee of the Red Cross (ICRC)
1
International Communication project
1
International Confederation of Midwives ICM
1
International Crisis Group
1
International Diabetes Federation (IDF)
1
International Diabetes Federation IDF
1
International Disability Alliance
1
International Disability and Development Consortium (IDDC)
1
International Disability and Development Consortium’s Inclusive Education Task Group
1
International Federation of Medical Students’ Associations (IFMSA)
1
International Federation of Red Cross and Red Crescent Societies (IFRC), World Health Organization (WHO)
1
International Federation of Red Cross and Red Crescent Societies, Geneva
1
International Federation of Red Cross And Red Crescent Societies, International Organization for Migration, World Health Organization, et al.
1
International Federation of Red Cross and Red Crescent Societies, Water and Sanitation Mission Assistant
1
International Federation of Red Cross and Red Crescent Society (IFRC)
1
International Food Policy Research Institute
1
International Harm Reduction Development Program (IHRD)
1
International HIV/AIDS
1
International HIV/AIDS Alliance
1
International I nitiativ e for Impact E valuation (3ie)
1
International Initiative for Impact Evaluation (3ie)
1
International Institute for Environment and Developmend (IIED)
1
International Journal of Adolescence and Youth
1
International Journal of Behavioral Science
1
International Journal of Clinical and Health Psychology
1
International Journal of Current Research
1
International Journal of Development Research
1
International Journal of Health Policy and Management
1
International Journal of HIV/AIDS Prevention, Educa tion and Behavioural Science
1
International Journal of Molecular Scienes
1
International Journal of Sociology and Anthropology
1
International Journal of Tubercolosis and Lung Disease
1
International Journal of Vaccines and Vaccination
1
International Labor Organization (ILO)
1
International Livestock Research Institute (ILRI)
1
International Livestock Research Institute ILRI
1
International Medical Corps (IMC)
1
International Medical Corps IMC
1
International Organization for Migration (IOM)
1
International Pediatric Nephrology Association (IPNA)
1
International Pharmaceutical Federation
1
International Physicians for the Prevention of Nuclear War (IPPNW), World Medical Association, World Federation of Public Health Associations, International Council of Nurses
1
International Plannes Parenthood Foundation IPPF
1
International Plant Nutrition Institute, International Fertilizer Industry Association
1
International Primary Care - Respiratory Group
1
International Primary Care Respiratory Group
1
International Primary Care Respiratory Group (IPCRG)
1
International Primary Care Respiratory Group IPCRG
1
International Rescue Committe
1
International Rescue Committee (IRC)
1
International Rescue Committee, London School of Hygiene & Tropical Medicine, Assosa Referral Hospital
1
International Research Institute for Climate and Society
1
International Research Institute for Climate and Society, World Health Organization
1
International Santé Info Solidarité (SIS)
1
International Society of Nephrology
1
International Union Against Tuberculosis and Lung Disease (The Union)
1
International Union Against Tuberculosis and Lung Disease (The Union), CORE Group
1
International Union for Conservation of Nature and Natural Resources (IUCN), World Health Organization (WHO)
1
International Union of Forest Research Organizations (IUFRO)
1
International Vaccine Access Center, Johns Hopkins Bloomberg School of Public Health
1
International Vaccines Task Force (IVTF)
1
InternationalPharmaceuticalFederation
1
Internationl Committee of the Red Cross ICRC
1
Internet Interventions
1
Internews
1
IOP Science
1
Iosue, S.
1
IPNI, IFA
1
IPPF (International Planned Parenthood Federation)
1
IPPF ESEAOR, UNFPA
1
IPPNW
1
Ipsos
1
IR3S
1
Iran J Public Health
1
Irarrazaval M., Norambuena P. et al
1
IRC
1
IRC, International Rescue Committee
1
Iribarren, S.
1
Irish Aid
1
Irish Penal Refurm Trust
1
Irmalita, D.A. Juzar, Andrianto, et al.,
1
Iroezindu, M.
1
Isaac Boyd, Kirtimayi Mishra, and Cassie Dummett
1
Isabell Schierenbeck, Peter Johansson, Lena M. C. Andersson, Dalena van Rooyen
1
Isabella Jean , Francesca Bonino
1
ISCTE IUL
1
Isha, R.
1
Issues in Educational Research
1
Istituto Superiore di Sanità (ISS)
1
Istivto Svpreriore di Santità
1
Italian Journal of Pediatrics
1
ITPC
1
IUCN (International Union for Conservation of Nature), KNCF (Keidanren Nature Conservation Fund)
1
Ivan Rocha Ferreira da Silva, Jennifer Ann Frontera, and Osvaldo Jose Moreira do Nascimento
1
IvanBastian, Martien Borgdorff, Tine Demeulenaere et al.
1
Izeta-Alberdi, A.
1
IZGA
1
Izibewule, J.H. et al.
1
Izquierdo J.
1
J Epidemiol Community Health
1
J Family Med Prim Care
1
J J Medicine
1
J Neurosci Nurs.
1
J Pharm Pharm Sci
1
J. Lentfer
1
J. Mariani, Ferrante D., Battistella G., et al.
1
J. A. Caminero, A. Van Deun, P. I. Fujiwara, et. al
1
J. A. Triccas, C. Counoupas
1
J. Amon
1
J. Atkinson, Y. Chartier, C.L.Pessoa-Silva, et.al
1
J. Ayieko, L. Abuogi, B. Simchowitz, et al.
1
J. B. Farhat
1
J. Baer
1
J. Begovac
1
J. Begovacc
1
J. Bhiman, F. Bongweni et al.
1
J. Boffa
1
J. Borghi
1
J. Borghi et al.
1
J. Brooks, A. Adams, N. Moraga-Lewy et al.
1
J. Bueno de Mesquita
1
J. Buntine
1
J. Burnett
1
J. Bushee
1
J. C. Butler, R. R. Redfield
1
J. C. Graves
1
J. Cairns
1
J. Caldwell
1
J. Cole A. Farlow and I. Petrikova
1
J. Crowley
1
J. D. Lundgren
1
J. D. Lundgren D. Raben
1
J. de Jesus Mari, D. Razzouk, R. Thara, et al.
1
J. Dee
1
J. Dewbre
1
J. Dieleman, L. Singh et al.
1
J. Dodos
1
J. Duodu
1
J. E Wright, N. Aksee, et al.
1
J. E. Greenlee
1
J. E. Haberer
1
J. E. Lawn
1
J. Edmeades, R. Hayes, G. Gaynair (International Center for Research on Women (ICRW))
1
J. Fäldt Wahengo
1
J. Ferdosy
1
J. Fol
1
J. Fourie
1
J. G. Scott
1
J. Gao
1
J. Gardel Valverde , I. Camara Morais et al.
1
J. Gardemann and A.M. Buschmann (2020)
1
J. Gaugler, Ph.D.
1
J. Hoover
1
J. Inchley
1
J. J. C. Nuttal, B. S. Eley
1
J. J. Fiol
1
J. J. N. Noubiap
1
J. Kahn, A.Mastroianni, and L.S. Parker
1
J. Kaner and S.Schaack
1
J. Katchanov
1
J. Kates, A. Wexler, et al.
1
J. Kayita, P. Musoke et. al.
1
J. King
1
J. Kiyono and H. Ram Parajuli
1
J. Kose
1
J. Kutzin
1
J. Langer and J. Slawomirski
1
J. LEGRAND, R. F. GRAIS, P. Y. BOELLE, A. J. VALLERON, and A. FLAHAULT
1
J. Lindeman
1
J. Lundgren
1
J. M Rey
1
J. M. Garcia Calleja
1
J. M. Humphrey
1
J. M. Rey. M. Irarrázaval
1
J. M. Scofield et al.
1
J. M. Somers
1
J. Njala
1
J. Noeske
1
J. O. Errecalde
1
J. Osborne
1
J. Painter, P. Douglas, et al.
1
J. Palacio-Vieira
1
J. Peebles
1
J. Perry, L. Palmer, P. Thom, et al.
1
J. Peter Figueroa
1
J. Pillay
1
J. Powell
1
J. R. Andrews, S. Basu, D. W. Dowdy, et al.
1
J. R. Busza
1
J. R. Rasolofomanana, J. P. Rakotovao, E. Bazant, et al.
1
J. Rech. Sci. Univ. Lomé (Togo), Centre de Formation en Santé Publique
1
J. Ripley
1
J. Ritsher
1
J. Robert, K. Mohamed Abass et al.
1
J. Roer,
1
J. S. Morrison and S. Brundage, Center for Strategic and International Studies (CSIS) Global Health Policy Center
1
J. Salwan
1
J. Sekulić
1
J. Slikker
1
J. Smith
1
J. Solorio
1
J. Stadler
1
J. Starling
1
J. Stover
1
J. Strang
1
J. T. Galea
1
J. Tjaden
1
J. Turan
1
J. Turner et al.
1
J. V. Ershova, G. V. Volchenkov, D. A. Kaminski, et al.
1
J. Villayzàn
1
J. Vujcic, L.Blum, and P.K.Ram
1
J. W. Eaton
1
J. Wasserheit, H. Schünemann, et cl.
1
J. Wiley Publisher
1
J. Wolf
1
J. Wolf, C. Corvalán, et al.
1
J. Woodring
1
J.-I. Cakalo
1
J.-P. Raynaud
1
J.-W. De Neve
1
J.Ang Henry and L. Hasek
1
J.D. Javakhishvili
1
J.de D. Barreto Segundo, G.Gonçalves da Costa, et al.
1
J.E. Suk, D. Fischer et al.
1
J.F.Oletta, M.J.González, et al.
1
J.Fisher
1
J.G. Shaffer
1
J.Hopman, Z.Kubilay, H.Edrees,T. Allen, B.Allegranzi
1
J.Hows
1
J.Kelly, M.VanRooyen, J.Kabanga, et al. (Harvard Humanitarian Initiative)
1
J.L. Hamel
1
J.Lundgren
1
J.M. Pescarini, A.F.Silva, et al.
1
J.M.Mangan, Z. Tillova, et al.
1
J.Monger
1
J.Mphande
1
J.O’Donovan, K. Kabali, C. Taylor, et al.
1
J.P. Souza
1
J.P.Valenzuela and E. Palaganas
1
J.Pei-Chen Chang
1
J.Pfeil, R. Kobbe, S. Trapp, C. Kitz, M. Hufnagel
1
J.S. Richards, et al.
1
J.Smith
1
J.t V. Rajand
1
Jabulani G. Kheswa
1
Jack, H.
1
Jackson, J., Kheng Heng, L., Eklund, G. et al.
1
Jacksona, A.
1
Jacob, N.
1
Jacobs Foundation
1
Jacobson, J. A.
1
Jacobson, J. et al
1
Jacobsonc, J. et al
1
Jahit S, David WD
1
Jahn, Albrecht
1
Jain, R.P., et al.
1
Jaiswal, A. & Gupta, S.
1
Jama Network
1
James Darcy, Jessica Alexander, Maria Kiani et al.
1
JAMIA Open
1
Jamie Bartram, Sandy Cairncross, Thomas Clasen et al.
1
Jamison, D.
1
Jamison, Dean T.
1
Jane N. Mutanga
1
Jane Phiri and John E Ataguba
1
Janho, L
1
Janiri, L.
1
Jannin J., Villa L.
1
Janoske M, Liu B, Sheppard B
1
Japan Committee for UNICEF (JCU)
1
Japan international cooperation agency JICA
1
Japhary, M.
1
Jara A., Undurraga E. A. et al
1
Jassat, W.
1
Jatho A., Mugisha N.M., Kafeero J. et al
1
JCI insight
1
Jeadran N. Malagon
1
Jean Paul Beyeme Ondoua
1
Jean-Pierre Coulaud, George Schmid, ИгорьТоскин et al.
1
Jemoon, P.
1
Jennings, B.
1
Jenny García, Gerardo Correa, Brenda Rousset
1
Jens Martens and Karolin Seitz
1
Jensen, C.
1
Jessica Dym Bartlett, Sheila Smith, Elizabeth Bringewatt
1
Jessica Hamblen
1
Jessica Meeker, Stephen Thompson, Inka Barnett
1
Jessica O'Dowd, Malcolm MacLachlan, Chapel Khasnabis, Priscille Geiser
1
Jessica O’Dowd, Hasheem Mannan, Joanne McVeigh
1
Jesus, G.S.
1
Jésuites d'Afrique de l'Ouest
1
Jha, Prabhat
1
Jiang, N. et al.
1
JIAS ( Journal of the International AIDS Society)
1
Jibril , A.
1
Jilian A Sacks, Elizabeth Zehe, Cindil Redick et al.
1
Jim Crabb, and Emma Razi
1
Jimann, N.S.
1
Jiménez, P.
1
Jiménez-Herrera M.F., Llauradó-Serra M., Acebedo-Urdiales S. et al.
1
Jindal, D.
1
Jing Liu-Helmersson , H. Stenlund, A. Wilder-Smith, et al.
1
JMIR Publication Advancing Digital Health and Open Science
1
JNCI: Journal of the National Cancer Institute
1
JNHRC
1
Jo Durham, Vanphanom Sychareun, Phonevilay Santisouk & Kongmany Chaleunvong
1
Joanna Busza
1
Joanna Raven, H. Wurie and S. Witter
1
Joe Schofield, Sarah Hess, Bandana Malhotra et al.
1
Jogerst, K.
1
Johan Velema & Huib Cornielje
1
Johannes Kepler University Linz
1
Johanniter-Unfall-Hilfe e.V.
1
Johansson, Emily White
1
John Beard, Alana Officer, Andrew Cassels et al.
1
John Cosgrave, Ben Ramalingam and Tony Beck
1
John Hopkins Bloomberg School of Public Health
1
John Hopkins Hospital antimicrobioal Stewardship Program
1
John K. et al.
1
John Kinsman
1
John R. Perfect, William E. Dismukes, Francoise Dromer, et al.
1
John Ryan Institute Center for Catholic Studies
1
Johnny, N
1
Johns Hopkins Center for a Livable Future
1
Johnson & Johnson
1
Johnson E. et al.
1
Johnson, P.
1
Johnson-Hanks J.
1
Johnstone, C.
1
Joint Call to Action for WASH in Schools
1
Joint Commissioning Panelfor Mental Health
1
Joint United Nations Programme on HIV
1
Joint United Nations Programme on HIV/AIDS (UNAIDS)
1
Jolliffe, Kim
1
Jones B. A., Grace D. et al
1
Jones I.
1
Jorge Emmanuel and Ruth Stringer
1
Jose Bertolote, José Miguel Caldas de Almeida, Thomas Bornemann et al.
1
Joseph J. Valadez and Babu Ram Devkota
1
Joseph K. Gona, Newton C.R., Hartley, Sally, et al.
1
Joseph Kutzin, Sophie Witter, Matthew Jowett et al.
1
Joseph M Rey,Tolulope T Bella-Awusah,Jing Liu
1
Joseph M. Rey, Francisco B. Assumpção Jr, Carlos A. Bernad, Füsun Çetin Çuhadaroğlu, Bonnie Evans, Daniel Fung, Gordon Harper, Loïc Loidreau, Yoshiro Ono, Dainius Pūras, Helmut Remschmidt, Brian Robertson, Olga A. Rusakoskaya, Kari Schleimer
1
Joseph McCord, Emily Bancroft and Jessica Crawford
1
Joseph Rowntree Foundation
1
Joseph, F. J.-J.
1
Josephine Ippe, Diane Holland, Leah Richardson, et al.
1
José A. Caminero
1
José, F.
1
Joshi, M.P.
1
Josi Salem-Pickartz
1
Joslin Dogbe, Ellis Owusu-Dabo, Anthony Edusei et al.
1
Journal des anthropologues
1
Journal of Acquired Immune Deficiency Syndromes (JAIDS )
1
Journal of Acquired Immune Deficiency Syndromes (JAIDS)
1
Journal of AIDS & Clinical Research
1
Journal of AIDS and HIV Infections
1
Journal of Allergy and Clinical Immunology: Global
1
Journal of Atherosclerosis and Thrombosis
1
Journal of Biosocial Science
1
Journal of Child and Adolescent Mental Health
1
Journal of Community Health
1
Journal of Cystic Fibrosis
1
Journal of Family Medicine and Disease Prevention
1
Journal of Fungi
1
Journal of Health Monitoring
1
Journal of Immunology, Infection & Inflammatory Diseases
1
Journal of Infection and Public Health
1
Journal of International Development
1
Journal of Microbiology and Infectious Diseases
1
Journal of Movements Disorders
1
Journal of Neurology and Neuroscience
1
Journal of Nursing Care
1
Journal of Palliative Medicine
1
Journal of Pharmaceutical Policy and Practice
1
Journal of Psychiatry
1
Journal of the American Academy of Child & Adolescent Psychiatry
1
Journal of the American Heart Association
1
Journal of the Brazilian Society of Tropical Medicine
1
Journal of the International AIDS Society (JIAS)
1
Journal of Trauma and Critical Care
1
Journal of Tropical Diseases
1
Journal of Tuberculosis Research
1
Jovicic, J.
1
Jowett, M.
1
JSI
1
JSI Research & Training Institute
1
JSI Research & Training Institute, Inc., and Management Sciences for Health
1
JSI Research & Training Institute, Inc., et Management Sciences for Health
1
Juanid, E.
1
Judith Baart, J., and F. Taaka
1
Juga, E.
1
Julia D Machado,Arthur Caye,Paul J Frick et al.
1
Julián-Jiménez, A.
1
Juliette Raymond
1
Julio C Padilla
1
Junitos pelo fin da Tuberculose
1
Juodkaite D.
1
Jusot, V.
1
Jürg Barben, Christoph Berger, Erik C. Böttger, et al.
1
K. Slobodianiuk
1
K. A. Holloway, World Health Organization (WHO)
1
K. A. Thomson
1
K. Achebe
1
K. Asedeu
1
K. Asiedu
1
K. Boegel
1
K. Butler
1
K. Church
1
K. Cranston, A. DeMaria (Bureau of Infectious Disease)
1
K. Davtyan, H. Davtyan, et al.
1
K. Dickson
1
K. Doerholt
1
K. Freeborn
1
K. G. Andrews
1
K. Green
1
K. Greenblott
1
K. Gryboski, N.V. Yinger
1
K. H. Mayer
1
K. H. Onarheim, M. Taddesse, O. F. Norheim, et al.
1
K. Hagmaier
1
K. Hauck
1
K. Hiban, I. Frost, et al.
1
K. Hill
1
K. J. Zucker
1
K. Khalid, A.Wharton-Smith, et al.
1
K. Kleineidam, L.Bakken, et al.
1
K. Kruja
1
K. Kulik and U.Binder
1
K. Lancaster
1
K. Lauer
1
K. Lindner
1
K. Malinowska-Sempruch
1
K. Ördek
1
K. P Msyamboza, L.Mawaya 2 , H.W Kubwalo, et al.
1
K. Runions
1
K. Saito
1
K. Schenkel, T. Bauer
1
K. Sorsdahl
1
K. Stone
1
K. Suzuki, R. E. Simmonds et al.
1
K. Tehoungue
1
K. Tolksdorf
1
K. vinh quoc Luong, L. T. H. Nquyen
1
K. Vinke
1
K. Wallner
1
K. West Slevin
1
K. Wilson
1
K. Zok, and F. Faulbaum
1
K.Dheda, T. Gumbo, G. Maartens, et al.
1
K.K O’Brien
1
K.K. Iloh
1
K.L Tang, N.P Caffrey, D.B Nóbrega, et al.
1
K.L.Ebi
1
Kabare K.
1
Kabré, I. et al.
1
Kabue M., Kasungami D., et al. ,
1
Kadam. A.
1
Kadowa, Isaac
1
Kadridin Pirov, Umriniso Sirojiddinova, Oktam Bobokhojaev, et al.
1
Kafle KK., Karkee SB., Shrestha N., et al.
1
Kafle, Ramesh B., Komal P. Dulal, and Krishna P. Pandey
1
Kagisha, V.
1
Kah, C.
1
Kaiser Family Foundation
1
Kakkar M., Chatterjee P. et. al.
1
Kalafs.S.
1
Kalibala Samuel, Nrupa Jani and Getachew Kassa
1
Kalksma-van Lith, B. , Graaff, D. de
1
Kalla, I.S.
1
Kallam, B.
1
Kallander, K.
1
Kaloti R., R. Kafri, H. Meghari
1
Kamal Narayan Kalita, Jyoti Hazarika, Mohan Sharma, et al.
1
Kamala Achu, Kathy Al Jubah, Svein Brodtkorb, Philippe Chervin, Peter Coleridge, Mike Davies, Sunil Deepak, Kenneth Eklindh, Ann Goerdt, Cindy Greer, Karen Heinicke-Motsch, Derek Hooper, Venus B Ilagan, Natalie Jessup, Chapal Khasnabis, Diane Mulligan, Barbara Murray, Alana Officer, Francesca Ortali, Bob Ransom, Aline Robert, Sue Stubbs, Maya Thomas, Venkatesh Balakrishna et Roselyn Wabuge-Mwangi.
1
Kamali M, Munyuzangabo M, Siddiqui FJ, et al.
1
Kamali, M.
1
Kamradt, T., B.S. Kamps J. García-Rosales Delgado
1
Kang Yiu Lai, Wing Yiu George Ng and Fan Fanny Cheng
1
Kanu, H.
1
Kapa, D.R.
1
Kapiriri, L.
1
Kaplan, W.A.
1
Kapungwe, A.
1
Karagiannidis, C.
1
Karen Human Rights Group
1
Karen LeBan , Maryse Kok and Henry B. Perry
1
Karen Vilholth
1
Karen Weidert, Amanuel Gessessew, Suzanne Bellet al.
1
Karin Hatzold
1
Karina Casanova
1
Kariuki S., K. H. Keddy, M. Antonio
1
Karl le Roux, Ingrid M le Roux, Nokwanele Mbewu & Emily Davis
1
Karmali, D.
1
Karolina Stasiak & Sally Merry
1
Kasipo, Charles
1
Kasmera
1
Kasper, J.
1
Kate Kerber, Stefan Peterson & Peter Waiswa
1
Kates J,
1
Kates J.
1
Kathleen R Delaney, Janice L. Cooper & Sylvia Nshemerewire
1
Katholische Hochschule NRW KatHo
1
Katie Hayes, G. Blashki, J. Wiseman et al.
1
Katie Murphy, Sandra Maignant, Laura Boone, Sarah Smith
1
Kato-Wallace, J.
1
Katrin Leitmeyer
1
Katrin Oberndörfer
1
Katte, J.C.
1
Katz, R.
1
Kaushik, C.
1
Kavita Singh, Isaac Osei-Akoto, Frank Otchere et al.
1
Kayemba Nalwadda, Guwatudde D, Waiswa P, Kiguli J, Namazzi G, Namutumba S, Tomson G, Peterson S.
1
Kazyoba, P. et al.
1
Keil, U.
1
Kello, A.
1
Kelly L, Cooper M,
1
Kelly Puent
1
Kelsey Vaughan & Aradhana Thapa
1
Kementerian Kesehatan RI
1
Kementerian Koordinator Bidang Kesejahteraan Rakyat Republik Indonesia, Kementerian Kesehatan Republik Indonesia, et al.
1
Kementerian Menteri Kesehatan Republik Indonesia
1
KEMRI-Wellcome Trust Research Programme and African Academy of Sciences
1
Kengne, A.P. et al.
1
Kennedy, A.
1
Kenya Law Reports (KLR)
1
Kenya Medical Training College (KMTC)
1
Kenya Ministry of Public Health and Sanitation
1
Kenya Working Papers
1
Kenyan Red Cross Society
1
Ker K, Tansley G, Beec her D, Perner A, Shakur H, Harris T, Roberts I
1
Kerry L.D. MacQuarrie, Lindsay Mallick &
1
Kessler, R.C., Aguilar-Gaxiola, S., Alonso, J., et al.
1
Kestel, D., et al.
1
Kett, M.
1
Kevin Runions
1
Keymanthri Moodley, Kate Hardie, Michael J Selgelid, et al.
1
KFF
1
KFF - Henry J Kaiser Family Foundation
1
Khadka, B.B., Karki, Y.B.
1
Khairunisa Suleiman
1
Khalil, A.
1
Khan, Farzana
1
Khan, J.
1
Khan, J.A.
1
Khanal M. N., Shrestha D.R., Panta P.D., and Mehata S.
1
Khatri RB, Mishra SR, Khanal V, Gelal K and Neupane S
1
Khawar Sana, M.
1
Khazaei, Z.
1
Khdr Sabir, D. et al.
1
KHRG
1
Khuluza, F.
1
Kiarie H., Toweet J.
1
Kickbusch I.
1
Kigume, R.
1
Kiley, J.
1
Kim, A.
1
Kim, J.-J. et al. (Éd.)
1
Kim, M.S.
1
Kimani D., Mugo M., Kioko U. et al.
1
Kincaid-Smith, J.
1
Kinder- und Jugendpsychiatrie/-psychotherapie, Universitätsklinikum Ulm
1
King E. J., N. Zotova
1
King J. D.
1
King, J.D.
1
Kingdom of Swaziland Ministry of Health
1
Kings College London
1
Kingue S., Rosskam E., Bela AC., Adjidja A., Codjia L.
1
Kinuthia, J.
1
Kirakoya-Samadoulougou F., K. Jean, M. Maheu-Giroux
1
Kirenga, B.J.
1
Kirsten Thomson
1
Kishimoto T., Robenzadeh A, Leucht C, et al.
1
Kistnasamy, B.
1
Kitchin, O.
1
Kizito O and Juma F
1
Kleefeldt, E.
1
Klein O. et al
1
Kleynhans, J.
1
Klingenfeld D. , König C., et al.
1
Klinik für Kinder- und Jugendpsychiatrie/Psychotherapie des Universitätsklinikum Ulm
1
Klinik für Psychiatrie und Psychotherapie
1
Klinkenberg, E. & Ochola, R.
1
Kloeck, P. et al.
1
Klug, E. et al.
1
Kluge, S. et al.
1
KMC India Network
1
Knaepen, H.
1
KNCV TUBERCULOSIS FOUNDATION
1
Knipper, M.
1
Knoll, M.D.
1
Knowledge Translation Unit, et al.
1
Knowledge Translation Unit, Prefeitura Florianópolis, et al.
1
KNV
1
Kobusingye, Olive
1
Koch, L. et al.
1
Kochmann, J.
1
Kochmann, J., Klimpel, S.
1
Kocks, J.
1
Koenig, H.G.
1
Kohn R, Ali A, Puac-Polanco V, Figueroa C, López-Soto V, Morgan K, et al.
1
Kokki, M.
1
Kola L.
1
Komisi Penanggulangan AIDS
1
Kompetenznetz Public Health COVID-19
1
Kondowe, K. et al.
1
Konrad-Adenauer-Stiftung
1
Kontsevaya A, Farrington J, Balcılar M, Ergüder T
1
Kopittke, P.M.
1
Koren, H.
1
Korenromp E.
1
Korn, D.A. and H.J. Shaffer
1
Kostova, D. et al.
1
Koulidiati J. L., Nesbitt R. C., Ouedraogo N. et. al.
1
Kovacic, V.
1
Kraef, C.
1
Kraemer, J.
1
Kratz J.M.
1
Kratzel, A.
1
Kraus J.
1
Kraus J. et al.
1
Kraus, S.
1
Krause G., M. Borchert, J. Benzler et al.
1
Krause, S.
1
Kreienbrock, L. et al.
1
Krishna Hort, Valeria de Oliveira Cruz, Murad Sultan
1
Kristie L. Ebi, Joshua Nealon
1
Krupnick, Gary A.
1
Kruse, K.
1
Ku, Ya Lie
1
Kuepfer, I.
1
Kulkarni, S.
1
Kumar Roy., S. and S. Bhattacharjee
1
Kumar, M.
1
Kunda J., Gosling S., Foody G. et al.
1
Kunz, M.
1
Kuper, H.
1
Kurscheid, J.
1
Kwan, G.F.
1
Kwizera, R.
1
Kwonjune J. Seung, Michael L. Rich, Amy Elizabeth Barrera-Cancedda et al.
1
Kırmızı Şemsiye Cinsel Sağlık ve İnsan Hakları Derneği
1
L'avoisier
1
l.
1
L. A Graybill
1
L. Alfieri, M. Flörke et al.
1
L. Anderson and E. Hamblion
1
L. Anderson, PharmD
1
L. Aparecida de Souza Teles and E.G. da Silva Andrade
1
L. Bardfield
1
L. C. M. Lebreton, H. S. Carson et al.
1
L. Cai
1
L. Calhoun
1
L. Cibrelus
1
L. Cluver
1
L. Crigler
1
L. Crigler, et al.
1
L. Davies
1
L. Engelbert Bain
1
L. F. Owolabi
1
L. Fairlie
1
L. Ferguson
1
L. Geffen
1
L. Gerardo Castellanos
1
L. Guillermo Castañeda
1
L. Gujral, M. Benigna Matsinhe, M. Eusébio Luis, et al.
1
L. Hart
1
L. Imre, A. Lourenço, N. Ahamed, et al.
1
L. Jankelowitz
1
L. Jenkins, H. Swanepoel, et al.
1
L. L. Abuogi
1
L. Makszin and C.Jurberg
1
L. Marín-Léon
1
L. Messner, L. Crye
1
L. Mofenson
1
L. Morrison
1
L. Myer
1
L. N. Chigbu, C. U. Iroegbu
1
L. N. Patel,and A. K. Detjen
1
L. Napoles
1
L. Ndlovu
1
L. Oseni
1
L. Pandit
1
L. R. Augustemak de Lima
1
L. Richter
1
L. Rumble, A. A. Ramly, M. Nuryana, et al.
1
L. S. Saldanha, L. Buback, J. M. White, et al.
1
L. Savioli
1
L. Schestag
1
L. Schölin
1
L. Sharvadze
1
L. Soutongonoma, L. Ouédraogo et al.
1
L. Sturua
1
L. Sulaberidze
1
L. Telisinghe, K. L. Fielding, J. L. Malden, et al.
1
L. Teplitskaya
1
L. Xu
1
L. Zhou
1
L.-A. Long
1
L.-G. Bekker
1
L.A. Chimoy and C. Tunoque
1
L.E. Escobar, R. Lowe et al.
1
L.Houétondji Codjo, D. Dokoui, S, et al.
1
L.R. Huntoon,
1
L.S.
1
La Grutta, S.
1
La Revue Médicale de Madagascar
1
La Sociedad Argentina de Infectología S.A.D.I.
1
Laaser, U., F. Beluli
1
Labbé, T.
1
Labonté et al
1
Lacy-Nicholas, J.
1
Ladnaya, N.
1
Laech-Kemon J.
1
Laili Irani, Sara Pappa, and Pierre Dindi
1
Laisure, M.
1
Lalloo, U.
1
Lalloo, U.G.
1
Lambert, V.
1
Lambert, V. et al.
1
Lamine Diouf, M.
1
Lammie, P.
1
Lamontagne E.
1
Lamontagne, F.
1
Lamunu M, Lutwama J.J, Kamugisha J
1
Lanari L., K. Y. Poli dos Santos
1
Lancaster, C.L., Teeters, J.B., Gros, D.F., Back, S.E.
1
Lancet 2017;
1
Lancet Glob Health
1
Lancet Oncology Commission
1
Landrigan, P.J.
1
Langston, A., Weiss, J., Landegger, J., et al.
1
Langwenya, Nontokozo
1
Lankoande M., P. Bonkoungou, S. Traore et al.
1
Lareau S.C., Fahy B. et al
1
Larmarnage J., Vallo R., Yaro S. et. al.
1
LaRocque, R.
1
Larrson, I.
1
Larson, E.
1
Larson, M. C.
1
Larson, P. S.
1
Laura Gover, Andrew Anguko, Jane Bruce, Godfrey Magumba, et al.
1
Laura Ortíz, Omar D. Bello, Liudmila Ortega et al.
1
Laurant M, van der Biezen M, Wijers N et al.
1
Laurence Cibrelus
1
Lawrence Flick Memorial Tuberculosis Clinic, Philadelphia Tuberculosis Control Program
1
Lawrence Mayega, Michel M. Dione, Brian Kawuma, et al.
1
Lawrence, E.
1
Layaye, D.
1
Leach, M.
1
Leach-Kemon, K.
1
LEAP
1
Lecovitz, E.
1
Ledikwe, J.H., Kejelepula, M., Maupo, K., et al.
1
Ledingham, K.
1
Lee J. Y., Marotzke J., et al.
1
Lee, J.H.
1
Lee, V.
1
Leibtag, S.
1
Leidi Herrera
1
Leisenheimer, M.
1
Lelieveld, J.
1
LeMier, Ryan
1
Lenney, W.
1
Lenzen, M.
1
Leon-Velarde, F.
1
Leonard Cheshire Disability and Inclusive Development Centre, UCL
1
Leong, T. L.
1
Leonova, N.
1
Les pressen universitaires de Yaounde
1
Lesosky, M.
1
Leufkens, H.G.M. et al.
1
Levy, Marcy, Veronica Magar, and Derrick Sialondwe
1
Lewis, E.
1
Léger, E.
1
Li Z., Richter L., Lu C.
1
Li, J.T
1
Libby Cohen
1
Liberia Medicines and Health Products Regulatory Authority (LMHRA)
1
Liberty O. Yaneza, Ma. Consolacion Dolor-Torres, Sue Ann R. Locnen
1
LIC. VILA UNSIHUAY LILA
1
Liese B
1
Lievens, T., Serneels, P. & Butera, D.
1
Lifebox and Ariadne Labs
1
Lifting the Burden
1
Limaya, R.J.
1
Lin V.
1
Lin, J.
1
Lin, Y., et al.
1
Lind, J. and Ndebe, J.
1
Linda Rudolf, Julian Caplan et al
1
Linda Young Landesman,
1
Lindsay, Daniel et al.
1
Lingo4you GbR
1
Linju Maria, J.
1
Lipsky A., Mulaki A., Williamson T., et al.
1
Lipton, J.
1
Lisa Myers, Laura Theytaz-Bergman
1
Liu Xiaoyun
1
Liverpool School of Tropical Medicine
1
Lloyd, Linda
1
Lloyd, Peter J.
1
Lloyd-Jones, Tony
1
Llyod, A.
1
Locher, F.
1
Lockwod DN.
1
Lode, H.
1
LOGICA Study Series
1
LOGICA, HHI
1
Logothetis, E.
1
Logunov, D.Y, et al.
1
London School of Hygiene & Tropical Medicine
1
London School of Hygiene & Tropical Medicine and CBM
1
London School of Hygiene and Tropical Medicine and the Technische Universität München
1
London School of Hygiene and Tropical Medicine, International Centre for Evidence in Disability, Plan International
1
Longo J. de Dieu
1
Lopez-Bernus, A. et al
1
Lorenzoni, C
1
Loua, A.
1
Louka, C.
1
Lowey, S.E.
1
López, L.
1
López-Bernús, A.
1
López-Jiménez, F.
1
López-Loyo, E.
1
LSHTM
1
LSVD
1
Lu C., Li Z.
1
Lubit, R.H. & Giardino, E.R.
1
Lucena Alves, C.P. de
1
Lucerne University
1
Lucile Peynot
1
Lucille Bartholomeusz
1
Ludwig,S., I.Kickbusch and R. Datt
1
Luitel N.
1
Lukito, A.A., A.U. Rahajoe, L.I. Rilantono, et al.,
1
Lukoye Atwoli, David Ayuku, Joseph Hogan, Julius Koech, Rachel Christine Vreeman, Samuel Ayaya, Paula Braitstein
1
Lund, C.
1
Lunds Universitet
1
Lungu, K.
1
Lutje, V.
1
Lúcia Rotenberg,1 Aline Silva-Costa,1 and Rosane Härter Griep
1
Lyle R. Petersen, M.D., M.P.H., Denise J. Jamieson, M.D., M.P.H., Ann M. Powers, Ph.D., and Margaret A. Honein, Ph.D., M.P.H.
1
Lynn Cockburn, Timothy N. Fanfon, Alexa Bramall et al.
1
L’Union Africaine des Aveugles (U AFA), Association Nationale des Aveugles du Cameroun (ANAC
1
M Mostafa Zaman
1
M.
1
M. A. Babu
1
M. A. Gasper, A. C. Hesseling, I. Mohar, et al.
1
M. A. Jiménez
1
M. A. Pallansch
1
M. Abebe
1
M. Allen
1
M. Aman
1
M. Angriman
1
M. Auton
1
M. B. Mello.
1
M. B. Ruíz
1
M. Ba, B. Camara et. al.
1
M. Ballard, Bancroft E., Nesbit J., et al.
1
M. Banda-Chalwe
1
M. Berry
1
M. Botticelli (Bureau of Substance Abuse Services)
1
M. Bray, M.S.Hirsch, D.Mitty, et al.
1
M. C. D. N. Vodouhe, L. Fakambi
1
M. Camacho
1
M. Cayemittes
1
M. Cheng
1
M. Corroon
1
M. Cotton
1
M. Couldrey
1
M. D. S. de Latini
1
M. Dara, C. D. Acosta, M. V. S. Vinklers Melchers, et al.
1
M. Dara, C. D. Acosta, V. Rusovich, et al.
1
M. Dara, I. Solovic, G. Sotgiu, et al.
1
M. Dara, M. Grzemska, M. E. Kimerling, et al.
1
M. Dara, O. Gozalov, O. Javadli, et al.
1
M. Djibuti
1
M. Do
1
M. Doara, D. Choroliani, P. de Colombani
1
M. E. Balcells, S. L. Thomas, P. Godfrey-Faussett, et al.
1
M. F. Biudes
1
M. F. Silveira
1
M. Fatuma Busangu, J.de Dieu Bizimana, et al.
1
M. Fendt-Newlin, S. T. Al-Harahsheh, et al.
1
M. Forßbohm, W. Haas
1
M. Fritzsche
1
M. G. Whitfield, H. M. Soeters, R. M. Warren, et al.
1
M. Gaanderse
1
M. Gallardo, et al.
1
M. Gaventa
1
M. Ghidinelli
1
M. Giles
1
M. Gjergji
1
M. Gogia
1
M. Golichenko
1
M. Gomes
1
M. Gottfredsson
1
M. Gutmann
1
M. Halla
1
M. Hammer
1
M. Hart
1
M. Herson
1
M. Higgins-Biddle
1
M. Hodaj
1
M. Hoekstra
1
M. Hoenigl
1
M. Idrissova
1
M. J. Abzug
1
M. J. D. Jordans
1
M. J. Sagrado
1
M. J. Stirratt
1
M. J. van der Werf, J. P. Zellweger
1
M. J. van der Werfa
1
M. Janier, V. Hegyi, N. Dupin et al
1
M. Joffres
1
M. K. Kumwenda
1
M. K. Sugai et al.
1
M. Kan
1
M. Kontio
1
M. L. Baranne
1
M. L. Belfer
1
M. L. Molag
1
M. L. Scanlon
1
M. Langer
1
M. Lefebvre
1
M. M. Ahmmed
1
M. M.L. dos Santos
1
M. Malecela
1
M. Manova
1
M. Marella and A. Robinson
1
M. Martin
1
M. Martínez-Álvarez et al.
1
M. Marume, et al.
1
M. Maruva
1
M. Mayan
1
M. Miller, K. Likjedahl, et al.
1
M. Mntonintshi
1
M. Motlaleng, J. Edwards, J. Namboze, et al.
1
M. Muno, et al.
1
M. Munyeme and S. Malama
1
M. Muñoz
1
M. Nakamura
1
M. Ndinakie Yakum, A. Pascal Goura
1
M. Nebuloni
1
M. Newman Owiredu
1
M. Nyamazana, G. Koyi, P. Funjika and E. Chibwili
1
M. Odhiambo Sewe, A.M Tompkins et al.
1
M. Outeda
1
M. Paz N. Marquez
1
M. Prescott, C. Boeke, T. Gotora, et al.
1
M. R. Jordan
1
M. Ramos-Ramirez
1
M. Ranganathan et al.
1
M. Rodríguez Buño, F.
1
M. Romanello, J. Rocklöv, et al.
1
M. Rose
1
M. Roser, P. Geldsetzer, T. Bärnighausen
1
M. S. Razai
1
M. S. Ruiz
1
M. Schneider
1
M. Schomaker
1
M. Semrau
1
M. Sharer, H. Cornman, et al.
1
M. Slutsker
1
M. Smelyanskaya, C. Daniels, et al.
1
M. Smelyanskaya, J. Duncan
1
M. Sologashvili
1
M. Sonego
1
M. Stockton
1
M. T. Schneider
1
M. Thorogood
1
M. van den Boom
1
M. van der Boom, S. Talevski
1
M. Vitoriaa
1
M. Wolny, P. Kubaszewski
1
M. Wong
1
M.-A. Davies
1
M.-R. B-Lajoie
1
M.A. Connolly, M. Gayer and S. Ottmani
1
M.Bakare
1
M.Biehl, R. Gütter ,et al.
1
M.E. Grillet, L .Villegas, J.. Oletta, et al.
1
M.G. BA, A.N. Mbodj, M. Sembene, A.D. Camara, A.A. Dia
1
M.J.
1
M.J. Choi
1
M.J. Chomba, S.G. Mukuria, P.W. Kariuki, S. Tumuti, B.A. Bunyasi
1
M.J. Nieuwenhuijsen, M. Gascon
1
M.Johnson
1
M.Lyman, M.J. Stucke, et al.
1
M.M. Bailey, D. Bickford et al.
1
M.M.M. Kabamalan and E.P. Laguna
1
M.N. Ngongondo
1
M.Owen-Smith, et al.
1
M.R. Rajagopal Vallath Nandini, Lulu Mathews, et al.
1
M.Revishvili
1
M.S. Jellinek and J. M. Murphy
1
M.S. Ngoma
1
M.S. O’Shea, J. M.Girón, L. Cabrera, et al.
1
M.Sergio, R.E. Paiva Souto and J.Segata
1
M.W. Robinson
1
Ma. B. Alves de Souza
1
Maailma Terviseorganisatsioon (Euroopa)
1
Mabakutuvangilanga Ntela, S.-D., Morvillers, J.-M., Goutte, N. et al.
1
Macedonian Journal of Medical Sciences
1
Machado, J.D.
1
Machalaba
1
Machalaba, C.
1
MacKinnon, K.
1
MacKinnon,K.
1
Macklin, M.
1
Maclean Soruco, Enrique y Eguivar, Mario A
1
MacNeill A.
1
MacQuarrie, Kerry L.D., Sarah E.K. Bradley, Alison Gemmill, and Sarah Staveteig
1
Madhukar Pai
1
Madkour, A.
1
Magagula, Samuel V.
1
Magalhães, C.R.
1
Mageni, Judith Nekesa, Ann Mwagni, Samwel Mbugua, and Vincent Mukthar
1
Magezi, V.
1
Magitta, N.F.
1
Maguire, B.
1
Maguire, B.J.
1
Magwenzi, P.
1
Mailloux, N.A. et al.
1
Maina T., Kirigia D.
1
Mair, L.
1
Mairie de Paris
1
Maite Ferrin
1
Majumdar, P. and Fagan, T.
1
Makanjuola, A. et al.
1
Makatjane, T. J., T. Hlabana, and E. M. Letete
1
Makhashvili, N.
1
Makingi G.
1
Makoka, Donald
1
Makumi, D.
1
Makwe, C.
1
Malaria No More
1
Malawi Government
1
Males, J.
1
Malgosia Grzemska, Elizabeth Mathai
1
Malich, G
1
Malik, A. A.
1
Mallick, Lindsay, Courtney Allen, and Rathavuth Hong
1
Mallick, Lindsay, Tukur Dahiru, and Kerry L.D. MacQuarrie
1
Mallick, Lindsay, Wenjuan Wang, Temsah, Gheda
1
Malou Adom P. V.1, Makoutode Ch. P.2, Gnaro T.3, Ouro-Koura A.-R.4, Ouendo E. M.5, Napo-Koura G.6, Makoutode M.7
1
Maluka, S.
1
Maman, D.
1
MAMI, Irish Aid, Eleanor Crook Foundation
1
Management Sciences for Health (MSH)
1
Management Sciences for Health (MSH) - Center for Pharmaceutical Management
1
Manas R. , Behera R., Satpathy S.K.
1
Mandrup, L. & Elklit, A.
1
Mangin, A.
1
Mangwiro, TNC.
1
Manjula Marella, Alexandra Devine, Graeme Ferdinand Armecin et al.
1
Manne-Goehler, J.
1
Manne-Goehler, J. et al.
1
Manolito L. Chua, Marissa M. Alejandria
1
Manual de Salud Mental Infantil y Adolescente de la IACAPAP
1
Manuel Sanchez-Montero and Núria Salse Ubach
1
MaoThao
1
Mapako, Tonderai, Simbarashe Rusakaniko, Maarten J. Postma, Marinus van Hulst, Janet Dzangare, Stellah Ngwende, John Mandisarisa, Ponesai Nyika, David A. Mvere, Owen Mugurungi, and Mufuta Tshimanga
1
Marc Prou & Mel Schorin
1
Marcella Deluca, Carlo Tramontano, Maria Kett
1
March of Dimes
1
Marchiol, A
1
Marchissio, E.
1
Marciani, D.J.
1
Marcus, M.E.
1
Margaret E. Greene and Andrew Levack
1
Margaret Grigg , Michelle Funk, Natalie Drew et al.
1
Margie Buchanan-Smith and John Cosgrave
1
Maria A Zuurmond, Ilias Mahmud, Sarah Polack, Jenny Evans
1
Maria das Graças Wanderley de Sales Coriolano
1
Maria del Carmen Casanovas, Knut Lönnroth, Luz Maria De-Regil et al
1
Maria Droste, Dr. Ali Kemal Gün, Hedwig Kiefer, et al.
1
Maria Faurholt-Jepsen, Michael Bauer and Lars Vedel Kessing
1
Maria Jakovljevic & Sheryl Buckley
1
Maria Neira, Edward Kelley, Mickey Chopra et al.
1
Maria Virginias Villegas
1
Maric F., Chance-Larsen K., Chevan J. et al.
1
Marie-Luise Abshagen, Anna Cavazzini, Laura Graen, Wolfgang Obenland
1
Marieke Boersma
1
Marina Smelyanskaya, John Duncan
1
Marini Ísola, A.
1
Marino J. González R., Elena M. Rincón O.
1
Mario R Dal Poz, Neeru Gupta, Estelle Quain and Agnes LB Soucat
1
Marissa Vicari
1
Maritim, P., A. Silumbwe, J.M. Zulu, et al.
1
Maritza Padrón-Nieves, Wilmer Alcázar, Alicia Ponte-Sucre
1
María de Lurdes Cartaya
1
María Eugenia Grillet, Fabiola Del Ventura
1
María Eugenia Landaeta
1
Mark F. Cotton
1
Mark Newton Stella A. Eguma Olamide O. Dairo
1
Mark W. Rosegrant | Jawoo Koo | Nicola Cenacchi
1
Mark, A.
1
Markbreiter, J.
1
Marks, S. et al.
1
Maroufou Jules Alao, Blaise Ayivi and Didier Lacombe
1
Marschall P., S.Flessa
1
Marsela Robo
1
Marselle M., Stadler J., Korn H., et al.
1
Marselle, M.R.
1
Marten, R.
1
Martin Kayitale Mbonye, Sarah M Burnett, Robert Colebunders, et al.
1
Martin, D. et al.
1
Martina Drescher (Université de Bayreuth)
1
Martinez Viciana, C.
1
Martinez, E.
1
Martinez, L.
1
Martinez, ML et al.
1
Martinez-Alvarez M.
1
Martinez-Alvarez M. et al
1
Martinez-Portilla r.J.
1
Martínez-Austria Polioptro,F and Bandala E. R
1
Marty, F.M.
1
Marvin L. Birnbaum
1
Marx, N.
1
Mary De Silva, Lucy Lee& Grace Ryan
1
Mary Florence Mukisa
1
Mary Kay Kindhauser, Tomas Allen, Veronika Frank, et al.
1
Mary-Ann Waddell & Rob Aley
1
Mary-Anne Hartley, Alyssa Young, Anh-Minh Tran et al.
1
Maryland, USA: ICF International
1
Mas, F.
1
Masa
1
Masibo, Peninah K
1
Massachusetts Department of Public Health
1
Massachusetts General Hospital
1
Massard da Fonseca, E.
1
Massoda Tonye, S.G.
1
Masson-Delmotte, V.
1
Masumbuko ClaudeK, Underschultz J,Hawkes MT
1
materia socio-medica
1
Maternal & Childhealth Advocacy International (MCAI) , Advanced Life Support Group (ALSG)
1
Maternal and Child Health Integrated Program (MCHIP)
1
Maternal and Child Health Integrated Program, US Aid du peuple americain
1
Maternal and Child Survival Program
1
Maternal Health Committee of the National Department of Health (NDoH) South Africa
1
Maternal Health Division Department of Family Welfare Government of India
1
Maternal Health Division Department of Family Welfare Ministry of Health & Family Welfare Government of India
1
Maternal Health Division Ministry of Health and Family Welfare Government of India
1
Mathauer, I.
1
Mathew Sunil George, Shradha Pant, Niveditha Devasenapat, et al.
1
Mathieu Maheu-Giroux, Lawrence Joseph, Patrick Belisle and others
1
Matsushita, K.
1
Matthew Benage
1
Matthew Hodes and Susan Gau
1
Mattinen, Hanna
1
Mauder, S., K. Geffert
1
Maurice Bucagu, Jean M. Kagubare, Paulin Basinga, Fidèle Ngabo, Barbara K Timmons & Angela C Lee
1
Maurice T. Agonnoude, François Champagne, Nicole Leduc
1
Mavi Alcántara, Maravillas Castro, Antonia Martínez, Visitación Fernández, & Concepción López-Soler
1
Mawa, P.
1
Maxwell, D. & Burns, J.
1
May L., K. Yadav, S. D. Gaona
1
Málaga, G.
1
Mäser, P.
1
Mbassi Awa,H.D.
1
Mbatchou Ngahane, B.H.
1
MBC Public Health
1
Mbengue M. A. S., A. K. Bei, A. Mboup
1
Mbengue M.A.S., Moussa S., Papa A. D. et. al.
1
Mboggo, E.
1
Mbugua S., L. D. MacQuarrie K.
1
Mburu, Gitau
1
Mc Gain F.
1
McCarthy J.
1
McCaula, M.
1
McCreanor, J.
1
McDaid, D.
1
McDonnell, J.
1
McGeown, J.
1
McGill University - Medical Foundation Series
1
McGloin, J.
1
McKee, M.
1
McKeon, G.
1
McKimm J., Redvers N., El Omrani O., et al.
1
McLean M., Gibbs T., Mc Kimm J.
1
Md. Akramul Islam, Susumu Wakai, Nobukatsu Ishikawa, A.M.R. Chowdhury, J. Patrick Vaughan
1
MDPI
1
MDPI Antibiotics
1
MDPI Journal of Clinical Medicine
1
MDPI Tropical Medicine and Infectious Disease
1
Measles Initiative
1
Measures, et al.
1
MedCrave
1
Medecins Sans Frontieres
1
Medecins Sans Frontieres (Access Campaign)
1
Medecins Sans Frontiers, Министерство здравоохранения Республики Таджикистан
1
MedGrave
1
medicaidmentalhealth.org
1
Medical Journal of Zambia
1
Medical Principles and Practice
1
Medical Protection Society
1
Medicine
1
Medicines Control Authority of Zimbabwe (MCAZ) | Ministry of Health and Child Care
1
Medicines Control Council (MCC), Department of Health Republic of South Africa
1
Medicus Mundi International Network (MMI)
1
Mediendienst Integration
1
Medina-Rincón, G.
1
Mediscript Ltd
1
Mediterranean Journal of Social Sciences MCSER Publishing, Rome-Italy
1
Medizin Fokus Verlag
1
medmissio
1
Medmissio Institut
1
Medscape
1
Meershoek A, Zwerling A, Daftary A, Citro B, Smyth C, Lewis D
1
Megan Best, Carlo Leget, Andrew Goodhead and Piret Paal
1
Megan S. Towle, et al.
1
Mehari, Asmeret Moges
1
Mehner-Gentner, J.
1
Mehta, M.K.
1
Mehtonen, J.
1
Meike J. Schleif, Iain Aitken , et al.
1
Melanie Duncan, et al.
1
Melissa Leach
1
Mellor, Steven
1
Melvyn Freeman, Michelle Funk, Soumitra Pathare et al.
1
Memorias do Instituto Oswaldo Cruz
1
Mendes L. da Silveira, D. M.
1
Mendoza, G.
1
Menjívar Escalante, E.V.
1
Mensing, M.
1
Mental Health Program
1
Mental, Neurological, and Substance Use Disorders: Disease Control Priorities, Third Edition (Volume 4).
1
MEPs Mobilising for Diabetes
1
Merbs, S.
1
Mercado, S.
1
Mercedes M. Maicán V., Ángel Granado, Jesús Cedeño, et al.
1
Mercer County Community College
1
Mercer, E
1
Merck Manual Professional Version
1
Mercy Corps
1
Meresman, S.
1
Mesic, Anita
1
Mews, C.
1
Meya, D.B.
1
Meyer, M.
1
Meyers, W.
1
Meyfroidt, P.
1
Mèdecines sans Frontières MSF
1
Médecins Sans Frontières (MSF), Stop TB
1
Médecins Sans Frontières MFS
1
Mgode, G.
1
Mhamphi, G. et al.
1
MI. Troya,B. Bartlam, and C. A. Chew-Graham
1
Micah A.
1
Micah et al.
1
Micah, A.E.
1
Michael T. Osterholma, Kristine A. Moorea, Nicholas S. Kelley et al.
1
Michel Makoutodé, Fatoumata Diallo, Virginie Mongbo, Édouard Guévart, Léodégal Bazira
1
Michel, G.
1
Michelle Funk, José Miguel Caldas de Almeida, Natalie Drew et al.
1
Michielsen, J.
1
Michigan State University, USAID
1
Micronutrient Initiative
1
Middlehurst, A.
1
MIDEM
1
Migration Policy Institute
1
Mijnarends DM, Pham D, Swaans K, et al.
1
Milani, B.
1
Military Medical Research
1
Miller A.
1
Miller, C.
1
Miller, M. K.
1
Milligan H., Goodwin K., et al.
1
Mills A.
1
Mills, E.
1
Min de Salud Colombia
1
Minh D Pham
1
Minisisterio da Saude - Secretaria de Vigilância em Saúde Doença pelo Novo Coronavírus, Brasilia
1
Minister for Medical Services
1
Minister of Health Republic of Indonesia
1
Ministere de la Sante & Rwanda Biomedical Centre
1
Ministere de la Sante, Rwanda
1
Ministere de la Santé, Direction Nationale de la Santé Publique , Programme National de Lutte contre les Maladies Transmissibles, Bénin
1
Ministeria de Saude, Brasil
1
Ministeria de Saude, Brasil
1
Ministerial Advisory Committee on Antimicrobial Resistance National Dept. of Health, South Africa
1
Ministerio de Salud Pública y Bienestar Social. Dirección de Salud Integral de Niñez y Adolescencia, Paraguay
1
Ministerio da Saude (MISAU), Instituto Nacional de Estatística (INE) e ICF International (ICFI)
1
Ministerio da Saude Brasilia, Centro Colaborador do SUS
1
Ministerio da Saude do Brasil
1
Ministerio de Salud y Deportes Bolivia
1
Ministerio de Educacion Paraguay
1
Ministerio de Salud - Colombia
1
Ministerio de Salud Colombia
1
Ministerio de Salud de Chile
1
Ministerio de Salud Ecuador
1
Ministerio de Salud Lineamientos para el diagnóstico, abordaje en el período agudo y seguimiento post COVID-19 de niños, niñas y adolescentes Programa Nacional de Salud Escolar (PROSANE) y Sociedad Argentina de Pediatría (SAP)
1
Ministerio de Salud Nicaragua
1
Ministerio de Salud Publica
1
Ministerio de Salud Publica Paraguay
1
Ministerio de Salud Publica y Bienestar Social
1
Ministerio de Salud Publica, Santo Domingo
1
Ministerio de Salud Pública y Bienestar Social Paraguay: et al
1
Ministerio de Salud Pública y Bienestar Social, Organización Mundial de la Salud, et al.
1
Ministerio de salud pública y bienestar social, Organización Panamericana de la Salud, et al.
1
Ministerio de salud pública y bienestar social, Paraguay todos y todas, et al.
1
Ministerio de Salud Pública y Bienestar Social, Primus Inter Pares Paraguay
1
Ministerio de salud pública y bienestar social, UNICEF, et al.
1
Ministerio de Salud y Deportes Bolivia
1
Ministerio de Salud y Desarrollo Social. Argentina
1
Ministerio de Salud y Proteccion Social Bogota, Colombia
1
Ministerio de Salud y Protección Social Bogotá
1
Ministerio de Salud, Argentina
1
Ministery of Public Health, Thailand
1
Ministère de Santé Publique, Cameroun
1
Ministère de la Lutte contre le VIH/SIDA, Bangui, RCA
1
Ministère de la santé - Secrétariat général - Direction général de l'information et des statistiques sanitaires
1
Ministère de la Santé de Burkina-Faso
1
Ministère de la santé et de l'action sociale
1
Ministère de la santé et de l'action sociale (MSAS) Sénégal
1
Ministère de la Santé et de la Protection, République Togolaise
1
Ministère de la Santé et de l’Action Sociale - République du Sénégal
1
Ministère de la Santé et de l’Action Sociale et Ministère de la Justice
1
Ministère de la Santé Publique , PROGRAMME NATIONAL DE LUTTE CONTRE LA TUBERCULOSE
1
Ministère de La Santé Publique de Madagascar
1
Ministère de la Santé Publique et de la Population, Haiti
1
Ministère de la Santé Publique et de la Population (M.S.P.P.)
1
Ministère de la Santé Publique et de la Population (MSPP) Haiti
1
Ministère de la Santé Publique et de la Population (MSPP) Haiti, the Centers for Disease Control, and the World Bank.
1
Ministère de la Santé Publique et de la Population, Haiti, et al.
1
Ministère de la Santé Publique et de la Population, OMS
1
Ministère de la Santé Publique, Madagascar
1
Ministère de la Santé, Direction de la Santé de la Mère et de l’Enfant, République du Bénin
1
MInistère de la Santé, Direction Nationale de la Santé Publique, Programme National de Lutte contre le SIDA
1
Ministère de la Santé, République du Bénin r
1
Ministère du Plan et de l’Economie Institut Centrafricain des Statistiques et des Etudes Economiques et Sociales
1
Ministère du Plan et du Développement Institut National de la Statistique et de l’Analyse Économique (INSAE) Cotonou, Bénin
1
Ministério da Saúde (MISAU) e Institudo Nacional de Estatística (INE)
1
Ministério da Saúde (MISAU), Direcção Nacional de Assistência Médica (DNAM)
1
Ministério da Saúde - Programa Nacional de Controlo da Tuberculose
1
MINISTÉRIO DA SAÚDE DE MOÇAMBIQUE DIRECÇÃO NACIONAL DE SAÚDE DIRECÇÃO NACIONAL DE ASSISTÊNCIA MÉDICA
1
Ministério da Saúde Direcção Nacional de Saúde Pública Programa Nacional de Controlo da Tuberculose
1
Ministério da Saúde do Brasil, Secretaria Atenção à Saúde
1
Ministério da saúde secretaria de Vigilância em saúde departamento de Vigilância das doenças transmissíveis, Brasil
1
Ministério da Saúde, Direcção Nacional de Saúde Pública, Departamento de Epidemiologia,
1
Ministério da Saúde, Direcção Nacional de Saúde Pública, Direcção de Planificação e Cooperação
1
Ministério da Saúde. Secretaria de Vigilância em Saúde, Brasil
1
Ministra de Salud y Desarrollo Social, Argentina
1
Ministrerio das Saude do Brasil
1
Ministry of Agricultural Development
1
Ministry of Agriculture, Livestock and Fisheries
1
Ministry of Education, Rwanda
1
Ministry of Foreign Affairs and International Cooperation, Directorate General for Development Cooperation (DGDC)
1
Ministry of Gender, Labour and Social Development, Uganda
1
Ministry of Health & Family Welfare
1
Ministry of Health & Family Welfare (MoHFW), World Health Organization WHO
1
Ministry of Health & Family Welfare ,India
1
Ministry of Health & Family Welfare Government of the Peoples Republic of Bangladesh
1
Ministry of Health & Family Welfare India
1
Ministry of Health (Malawi), USAID, UNFPA, UNICEF, Save the Children International, Clinton Health Foundation
1
Ministry of Health (MoH), Micronutrient Initiative (MI)
1
Ministry of Health [Kenya], National AIDS and STI Control Programme (NASCOP)
1
Ministry of Health and Child Care & UNICEF
1
Ministry of Health and Child Care, Zimbabwe
1
Ministry of Health and Child Welfare
1
Ministry of Health and Family Welfare
1
Ministry of Health and Family Welfare & Indian Council for Medical Research
1
Ministry of Health and Family Welfare & Indian Council of Medical Research
1
Ministry of Health and Family Welfare - Government of India
1
Ministry of Health and Family Welfare, Bangladesh
1
Ministry of Health and Family Welfare, Directorate-General of Health Services, Mycobacterial Disease Control, National Tuberculosis Control Programme
1
Ministry of Health and Family Welfare, Government of the People's Republic of Bangladesh
1
Ministry of Health and Family Welfare, India
1
Ministry of Health and Family Welfare, Pakistan
1
Ministry of Health and Population
1
Ministry of Health and Population Nepal
1
Ministry of Health and Sanitation, International Centre for Eye Health, Sightsavers
1
Ministry of Health and Social Services Namibia
1
Ministry of Health and Social Services, Namibia
1
Ministry of Health and Social Services, Republic of Namibia
1
Ministry of Health and Social Services, Windhoek, Namibia
1
MINISTRY OF HEALTH AND SOCIAL WELFARE
1
Ministry of Health and Social Welfare in Liberia and the World Bank
1
MINISTRY OF HEALTH AND SOCIAL WELFARE National AIDS Control Programme
1
Ministry of Health and Social Welfare, Central TB Division, India
1
Ministry of Health and Social Welfare, Government of India
1
Ministry of Health and Social Welfare, Government of Lesotho
1
Ministry of Health and Social Welfare, Republic of Liberia
1
Ministry of Health and Wellness
1
Ministry Of Health Community, Development,Gender, Elderly And Children, the United Republic of Tanzania
1
Ministry of Health Ethiopia
1
Ministry of Health Jordan
1
Ministry of Health Kenya
1
Ministry of Health Malaysia
1
Ministry of Health Nepal, National Tuberculosis Center
1
Ministry of Health Republic of Indonesia, PT. Multi Area Desentralisasi Pembangunan
1
Ministry of Health Saudi Arabia
1
Ministry of Health The United Republic of Tanzania
1
Ministry of Health Uganda
1
Ministry of Health Uganda, WHO Uganda
1
Ministry of Health Vietnam
1
Ministry of Health, Botswana;
1
Ministry of Health, CDC, Futures, et al
1
Ministry of Health, Ethiopia
1
Ministry of Health, Kingdom of Cambodia
1
Ministry of Health, Kingdom of Swaziland
1
Ministry of Health, Liberia
1
Ministry of Health, Liberia, World Health Organization (WHO), and Centers for Disease Control and Prevention (CDC)
1
Ministry of Health, Madagascar
1
Ministry of Health, Ministry of Food and Agriculture, et al.
1
Ministry of Health, National Aids Control Council
1
Ministry of Health, Nutrition & Indigenous Medicine
1
Ministry of Health, Pakistan
1
Ministry of Health, Republic of Botswana
1
Ministry of Health, Republic of Kenya
1
Ministry of Health, Repulic of Uganda
1
Ministry of Health, Rwanda & Rwanda Biomedical Centre
1
Ministry of Health, Singapore
1
Ministry of Health, World Health Organisation (WHO), Roll Back Malaria
1
Ministry of Health. The Goverment of the Kingdom of Swaziland
1
Ministry of Law and Justice, India
1
Ministry of Local Government, Information and Social Affairs (Rwanda)
1
Ministry of Medical Services, Kenya
1
Ministry of Medical Services, Ministry of Public Health and Sanitation
1
Ministry of Public Health & Sanitation
1
Ministry of Public Health and Sanitation Kenya
1
Ministry of Public Health and Sanitation, Kenya
1
Ministry of Public Health and Sanitation, Ministry of Medical Services
1
Ministry of Public Health, Quatar
1
Ministry of State for Special Programmes (MSSP) and Ministry of Provincial Administration and Internal Security - National Disaster Operation Centre (NDOC), Kenya
1
Ministry of Women Empowerment and Child Protection Republic of Indonesia
1
Ministry of Women, children and social Welfare Nepal
1
Minja, N.W.
1
Minos Mouzourakis, Kris Pollet, Ruben Fierens
1
Minsalud
1
Minsitry of Health
1
MISAU
1
Misereor
1
Mishra, S.R.
1
Missionalia
1
Missionsärztliches Institut Würzburg
1
Misterio de Salud Peru
1
Mitchell, S. et al.
1
Mitra, S.
1
Mixed Migration Centre
1
Miyata, T. et al.
1
Mjelde, Marit
1
Mkoko, P.
1
Mmbaga, Elia John
1
Mme C. Owona
1
MNPI
1
Moazzam Ali
1
Mochtar, C.A., R. Umbas, D.M. Soebadi, et al.,
1
Mock C. N., Nugent R. et. al.
1
Mock, C et al
1
Mock, Charles N.
1
Modi, D., N. Dholakia, R. Gopalan, et al.
1
Moeti, M.
1
Mohamed, A.J.
1
Mohamed, S.F.
1
Mohammed A. , Putnis N. et al.
1
Mohammed Kabir, Zubair Iliyasu, Isa S Abubakar & Muktar H Aliyu
1
Mohan P. Joshi Malaïka Ludman Dan Kibuule, et al.
1
Moine, S.
1
Molinas Vega, J.
1
Molly J Ryan, Tamara Giles-Vernick, Janice E Graham
1
Mombasa City Council
1
Momenabadi, V.
1
Monde, N.
1
Moner-Girona, M.
1
Monica de Castellarnau and Velina Stoianova
1
Moniruzzaman, M.
1
Mont, D.
1
Monteath-van Dok, A., Gallinetti, J., Kuper, H., Zuurmond, M., Danquah, L., Wing, K., &
1
Monteiro , J.D.
1
Montelongo, A.
1
MONWANOU Djohodo Inès
1
Moo-llanes, D.
1
Moodie,R.
1
Moore A.
1
Moorhouse, M.
1
Moraes de Oliveira, G et al
1
Moran, M.
1
Morbidity and Mortality Weekly Report
1
Morbidity and Mortality Weekly Report MMWR
1
Moreas Morelli, D.
1
Moriyama TS, Cho AJM, Verin RE et al.
1
Morris, J.
1
Morrison-Métois, Susanna
1
Morse, J.M.
1
Mosler, G.
1
Moss, D.
1
Motaleb, Mohammad Abdul
1
Mottram, J.C.
1
Moudatsou, M.
1
Moungou Mbenda S.
1
Move Humanity
1
Mowbray, C.
1
Mörchen, M., Ormsby, G., Bonn, T.S. & Lewis, D.
1
Mörk, A-C.
1
MPact: Global Action for Gay Men’s Health and Rights
1
Mpairwe, A.
1
Mpairwe, H.
1
Mpe, M.
1
Mphahlele, R.
1
Mphahlele, R.E.
1
Mphande, M.
1
Mpofu, M., Semo, B., Grignon, J., et al.
1
mPowering Frontline Health Workers
1
MRC South Africa
1
MSF Access Campaign
1
MSF Médecins sans Frontières
1
MSF South Africa and Lesotho
1
MSH, USAID
1
Mshelbwala, P.
1
Msomi, N.
1
Msuya, Sia E., Juma Adinan, and Neema Mosha
1
Muga R., Ndavi P., Kizito P. et al.
1
Mugisha J.
1
Mujaddid
1
Mukaratirwa, S. et al.
1
Mukende, M.
1
Mukhtar A Adeiza, Abdullah A Abba, Juliana U Okpapi
1
Mukund Uplekar, Diana Weil, Hannah Monica Dias et al.
1
Muleta, A.J., R. Lappan, T. P. Stinear, et al.
1
Muller, Helgard et al.
1
Multicultural Centre for Women’s Health
1
Multicultural Mental Health Australia
1
Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC)
1
Multidisciplinary Digital Publishing Institute
1
Multidisciplinary Digital Publishing Institute MDPI
1
Multiple Sclerosis international federation
1
Mumbo, AA.
1
Mundy, M.
1
Munist, M., Santos, H., Kotliarenco, M.A., et al
1
Munro, J. et al.
1
Munro, Leonie
1
Muntean Al., Popa M.
1
Munthali, A. et al.
1
Munyamahoro M., J. Ntaganira
1
Munyaneza, F.
1
Munyua P., A.Bitek, E.Osoro
1
Muñiz F. J., de Casado G. C. , et al.
1
Muñoz-Sánchez, A.I.
1
Murni I. K., T. Duke, S. Kinney et al.
1
Murphy
1
Murphy, J.P.
1
Murray C.
1
Murray, C.A.
1
Murray, C.J.L. et al.
1
Murray, J.
1
Mursaleena Islam
1
Musaazi, J.
1
Musana, J.I.
1
Mutale W.
1
Mutuku, Andrew Kyalo
1
Muula, S. A. et al.
1
Muzammil and Lopes
1
Mücke, H.
1
Mücke, H.G. et al.
1
Müller, J.
1
Müller, Olaf
1
MW Sonderup, Y Pillay et al.
1
Mwaiyeghele, E. et al.
1
Mwambona, J.
1
Mwangi M., Mutua1 M.K., et al.
1
Mwangi, Annabel
1
Mya, Kyaw Swa, Aung Tin Kyaw, and Thandar Tun
1
Myers, J.
1
Myron L Belfer, Suzan Song
1
N. Abera, T. Saballa, et al.
1
N. Amann, M. Arnell, et al.
1
N. B Ilangaratne
1
N. B. Ahmed
1
N. B. Bellareet
1
N. B. Carbone
1
N. Bam
1
N. Bellare
1
N. Bolokadze, et al.
1
N. C. Rollins
1
N. D. Volkow
1
N. Davies
1
N. Forda
1
N. Friedrichs
1
N. Fujita et al.
1
N. G. Kiobi, S. N. Nebere, J. K. Karanja
1
N. González Méndez de Vigo, J. Karpenstein und F. Schmidt
1
N. Green
1
N. H. Ponters, A. P. Dores
1
N. J. Sagala, S. Sofyani, Supriatmo
1
N. K. Arora
1
N. K. Ngandu
1
N. Konduri, K. Sawyer, N. Nizova
1
N. Kumar
1
N. L. Soh
1
N. L. Soh
1
N. M. Shehu
1
N. Maennling et al.
1
N. Mdaka
1
N. Metrebian
1
N. N. Fido
1
N. N. Mannakkara
1
N. Nguyen
1
N. O'Brien, K. Flott, et al.
1
N. P. Singh
1
N. Petrosillo
1
N. R. Calles
1
N. Rakhmanina
1
N. Redverse
1
N. Reuge and D. Amaro
1
N. Singh et al.
1
N. Solé, A. Marco, M Escribano, A. Orcau, et al.
1
N. Talat, S. Perry, J. Personnet, et al.
1
N. Tavagnutti
1
N. Tohnain, E. Tamajong
1
N. Tsereteli
1
N. U. Okubadejo
1
N. Wekwete
1
N.Dean
1
N.K. Biritwum
1
N.Paul, T. Bärnighausen, P. Geldsetzer
1
Naciones Unidas
1
Naciones Unidas Derechos Humanos Paraguay
1
Naciones Unidas El Salvador
1
Naciones Unidas, EHP
1
NACO India
1
NACO, Department of AIDS Control
1
Nafti, S.
1
Naik, N.
1
Naik, V.
1
Nakagaayi, D.
1
Nalbandian, A.
1
Nam Aidsmap
1
Namutebi, M.
1
Nana Twum Danso, Uta Lehmann, Jennifer Nyoni et al.
1
Nance, N.
1
Nancy G Guerra, Ariel A Williamson, Beatriz Lucas-Molina
1
Nankinga, O.
1
Nantanda, R.
1
Narula, J.
1
NASTAD (National Alliance of State & Territorial AIDS Directors)
1
NASTAD Zambia
1
Nathan Grills, Lawrence Singh, Hira Pant, Jubin Varghese, GVS Murthy, Monsurul Hoq, Manjula Marella
1
Nathan J. Blanchet and Osei B. Acheampong
1
National Center for TB and Leprosy Control (CENAT) , Cambodia
1
National Academy of Medical Sciences
1
National Academy of Medicine
1
National Academy of Sciences of the USA
1
National Agency for Food and Drugs Administration and Control (NAFDAC), Nigeria
1
National Agency for the Control of AIDS (NACA), Government of Nigeria
1
National AIDS Commission (NAC) and Lesotho Correctional Services (LCS), Government of Lesotho
1
National AIDS Commission Liberia
1
National AIDS Commission MAlawi
1
National AIDS Commission of Liberia
1
National AIDS Control Organisation
1
National AIDS Control Organisation (NACO), Ministry of Health & Family Welfare, Government of India
1
National AIDS Control Organisation (NACO), Ministry of Health and Family Welfare (MOHFW), Government of India
1
National AIDS Control Organisation, Ministry of Health & Family Welfare , Government of India,
1
National AIDS Control Organization (NACO)
1
National AIDS Control Programme (NACP)
1
National AIDS Council, Zambia
1
National Association of People With HIV Australia
1
National Association of State Public Health Veterinarians Compendium of Animal Rabies Prevention and Control Committee
1
National Bureau of Statistics (NBS)
1
National Catholic Reporter
1
National Center for Emerging and Zoonotic Infectios Diseases
1
National Center for Emerging and Zoonotic Infectious Diseases Division of Vector-Borne Diseases (CDC)
1
National Center for HIV
1
National Center for PTSD
1
National Center for Responsible Gaming (NCR)
1
National Centre for AIDS and STD Control
1
National Centre for Disease Control
1
National Centre of Disease Control
1
National Child Traumatic Stress Network (NCTSN) & National Center for PTSD
1
National Clinical Guideline Centre
1
National Consensus Project for Quality of Palliative Care
1
National Council for Law Reporting with the Authority of the Attorney-General
1
National Department of Health (NDoH) South Africa
1
National Dept. of Health, South Africa
1
National Development Planning Commission (NDPC) & United Nations system in Ghana
1
National Directorate for Economy, Equality and Gender and UNICEF
1
National Drug Authority (NDA), Uganda
1
National Epidemiology Center Department of Health Philippines
1
National Health Accounts Cell Ministry of Health & Family Welfare Government of India
1
National Health Accounts Technical Secretariat, Ministry of Health and Family Welfare, Government of india
1
National Health Education, Info rmation and Communication Centre/ MoHP and The Population, Health and Development (PHD) Group.
1
National Health Mission (NHM), Ministry of Health & Family Welfare, Government of India
1
National Health Mission India
1
National Health Mission, Ministry of Health and Family Welfare, Government of India
1
National Institue of communicable Diseases, India
1
National Institute for Medical Research
1
National Institute of Environmental Health Sciences
1
National Institute of Health
1
NATIONAL INSTITUTE OF MALARIA RESEARCH NEW DELHI
1
National Institute of Mental Health & Neurosciences, Bengaluru India
1
National Institute of Statistics, Cambodia
1
National Institutes of Health
1
National Legal Services Authority India
1
National Leprosy Eradication Programme (NLEP), Ministry of Health & Family Welfare, Govt. of India
1
National LGBTQ Task Force
1
National Libary of Medicine
1
National Malaria Control Program (NMCP) [Liberia], Ministry of Health (MOH), Liberia Institute of Statistics and Geo-Information Services (LISGIS), and ICF
1
National Malaria Control Program - NMCP
1
National Malaria Control Programme (NMCP) [Sierra Leone], Statistics Sierra Leone, University of Sierra Leone, Catholic Relief Services, and ICF.
1
National Malaria Elimination Centre, Ministry of Health, Zambia
1
National Malaria Elimination Programme Federal Republic of Nigeria Abuja, Nigeria et al.
1
National Primary Health Care Development Agency
1
National Primary Health Care Development Agency, Abuja, Nigeria
1
National Primary Health Care et al.
1
National Rabies Programme
1
National Rural Health Mission
1
National Rural Health Mission, DOTS
1
National Sexual Violence Resource Center
1
National Statistical Office Zomba, Malawi
1
National TB
1
National TB Control Programme, Bangladesh
1
National Tripartite Committee
1
National Tuberculosis and Leprosy Programme Ministry of Health and Social Welfare, Tanzania
1
National Tuberculosis Center
1
National Tuberculosis Center, New Jersey Medical School
1
National Tuberculosis Centre, Global Fund
1
National Tuberculosis Control Program, Cambodia
1
National Tuberculosis, Leprosy and Lung Disease Unit, Ministry of Health, Kenya
1
National Union of Disabilities’ Organizations of Rwanda (NUDOR)
1
National University of Lesotho
1
National Vector Borne Diseases Control Programme
1
National Women's Council of Ireland
1
Nations Unies, Conseil d’administration du Programme des Nations Unies pour le développement, du Fonds des Nations Unies pour la population et du Bureau des Nations Unies pour les services d’appui aux projets
1
Nature
1
nature medicine
1
Nature Research
1
Nature Scientific Reports
1
Naumann, D.N.
1
Nauta, M. H.
1
Naveed, A.
1
NCBI
1
NCBI (National Center for Biotechnology Information)
1
NCTSN
1
Ncube, M.
1
Ndambo, M.K.
1
Ndarukwa, P.
1
Ndeezi, G. et al.
1
Ndetei D, Musyimi C, Musau A, Matoke L, Mutiso V
1
ndia State-Level Disease Burden Initiative Cancer Collaborators
1
Ndjepel J.
1
Ndlovu, N.
1
NED Foundation nurses volunteers
1
Neil M Ferguson, Daniel Laydon, Gemma Nedjati-Gilani, Natsuko Imai, Kylie Ainslie, Marc Baguelin, Sangeeta Bhatia, Adhiratha Boonyasiri, Zulma Cucunubá, Gina Cuomo-Dannenburg, Amy Dighe, Ilaria Dorigatti, Han Fu, Katy Gaythorpe, Will Green, Arran Hamlet, Wes Hinsley, Lucy C Okell, Sabine van Elsland, Hayley Thompson, Robert Verity, Erik Volz, Haowei Wang, Yuanrong Wang, Patrick GT Walker, Caroline Walters, Peter Winskill, Charles Whittaker, Christl A Donnelly, Steven Riley, Azra C Ghani.
1
Neligan, A. & Sander, J.W.
1
Neonatal Guideline Development Group, Ministry of Health & Family Welfare, India
1
Nepal Health Sector Support Programme
1
Nepal Journal of Obstetrics and Gynaecology (NJOG)
1
Nepal Ministry of Health and Population, UNICEF, J. Crum, et al.
1
Nepal Public Health Foundation
1
Nepal, Ministry of Health, National Centre for AIDS and STD Control
1
Nephal Ophtalmic Society
1
Nesheim, Ingrid
1
Net Hope
1
Netsayi Wekwete, Naomi, Hamfrey Sanhokwe, Wellington Murenjekwa, Felicia Takavarasha, and Nyasha Madzingira.
1
Netzwerk - Wiener Netzwerk gegen sexuelle Gewalt an Mädchen, Buben und Jugendlichen
1
Netzwerks Flucht, Migration und Behinderung
1
Neuron Review
1
Neuropsychiatric hospital, Aro, Abeokuta, Nigeria
1
New England Journal of Medicine
1
New York Times
1
Newcastle University
1
Newman C
1
Newman et al
1
Newman, C., Kabagwira, A., Scislowicz, J., et al.
1
Newman, C.J., de Vries, D.H., Kanakuze, J., et al.
1
NewsGuard
1
NFD-N (National federation of the disabled- Nepal)
1
NFPA-UNICEF Joint Programme on Female Genital Mutilation/ Cutting (FGM/C)
1
Ng, C.
1
Ngombo, A.V.
1
Nguyen T, Hellbuyck M & Halpern M.
1
Nguyen, T.
1
Ngwa, W.
1
Nhlema, B.
1
Niang M. S., R. Derwiche, B. Mbengue
1
NICE
1
Nichiimunya N.
1
Nicholas, J.J.
1
Nichols, B. E.
1
Nicholson, S., Clarke, A.
1
Nicole Ritz, Folke Brinkmann, Cornelia Feiterna-Sperling. et al.
1
Nidhi Singal
1
Niederberger, E.
1
Niederberger,E.
1
Nieto-Sanchez C., Hatley DM, Gijalva MJ., et al.
1
Nieuwenhuijsen, M.J.
1
Nigeria Centre for Disease Control
1
Nigeria Centre for Disease Control, Abuja, Nigeria
1
NIH Public Access
1
Niilo Mäki Institute
1
Nikiema J. B.
1
Nikiéma J. B., K. Djierro, J. Simpore et al.
1
Nikolaos Mastellos, Tammy Tran, Kanika Dharmayat et al.
1
Nisha Bhat, Peter H. Kilmarx, Freeman Dube, et al.
1
Nitsche, A.
1
Njim T., H. Makebe, L. Toukam, et. al.
1
Nkhalamba, L.
1
Nkhoma, L. et all.
1
Nkoa, F.C.
1
Nkomazana, O., Peersman, W., Willcox, M., et al.
1
Nkurunungi, G. et al.
1
Noel G. Macalalad, Ma. Cecilia G. Ama, Arthur B. Lagos et al.
1
Nomura S. et al.
1
Nomura, S.
1
Nonhlanhla Nxumalo, Jane Goudge & Lenore Manderson
1
Nonvignon J.
1
Noormahomed E, et al.
1
Nora Groce and Julia McGeown
1
Norad
1
Norsk institutt for vannforskning (NIVA)
1
North-West University, SA
1
Norwegian Ministry of Foreign Affairs
1
Norwegian Red Cross
1
Norwegian Refugee Council
1
Norwegian Refugee Council, UNHCR
1
Noto, S.
1
Noubiap, J.J.
1
Nougueret, M.
1
Nouvellet, P.
1
Nove A., Friberg I., de Bernis L., et al.
1
Novel Psychoactive Treatment UK Network (NEPTUNE)
1
Nozaki, I.
1
NPJ
1
NR Rau, Satish K Nayak
1
NRC
1
Ntusi, N.A.B.
1
Nuclear Threat Initiative (NTI) and the Johns Hopkins Center for Health Security (JHU)
1
Nuffield Council on Bioethics
1
Nugent, R.
1
Nugent, Rachel
1
Nugroho
1
Nunziata, K. R.
1
Nurcombe, B.
1
Nurkhayani, E., E. Setyowati and Y.H. Sandyatma
1
Nurse, J. et al.
1
Nutrition Education for New Americans project of the Department of Anthropology and Geography
1
NVBDCP
1
Nwe Ni Myint et al.
1
Nwokike J., Ludeman E., Thumm M.
1
NWP, Aqua for All,Kit Publisher et al.
1
Nyamsore, J
1
Nyamusore, J
1
Nyandwi, J.B: et al.
1
N’weti-Comunicação para Saúde, Malaria Consortium Moçambique, DPS-Nampula
1
O'Donovan, G.
1
O'Neill, D.
1
O'Sullivan, B.
1
O. Aderomilehin
1
O. Ajose
1
O. Bandmann
1
O. Drouin
1
O. Gureje & A. Alem
1
O. H. Okojie
1
O. M. Balakireva
1
O. Morozova, S. Dvoryak a , ∗ , Frederick L. Altice
1
O. Neyrolles (Institut de Pharmacologie et de Biologoie Structurale)
1
O. O. Ojo
1
O. O. Oshinaike
1
O. O. Ozoya
1
O. O. Simooyqa
1
O. Odumosu
1
O. S. Levina
1
O. Samoylova
1
O. T. Ranzani
1
Obago, Irene T
1
Obichukwu I., Kennedy J., Harmer A.
1
Obiezue, RN.
1
Observatoire des situation de déplacement interne, Conseil norvégien pour les refugiés
1
Observatorio Regional de Recursos Humanos de Salud
1
OCCA Services
1
Ocran Mattila, P.
1
ODI_ Humanitarian Policy Group
1
Odlum, A.
1
OECD Publishing
1
Office for the Coordination of Humanitarian Affairs (OCHA)
1
Official Journal of the Asian Pacific Society of Respirology
1
Oficina del Alto Comisionado de las Naciones Unidas para los Derechos Humanos (OACNUDH), et al.
1
Oficina Regional de la Organización Mundial de la Salud
1
Ofori-Adu P.
1
Ogden Stephanie et al
1
Ogden, S.
1
Ogden, S., Gallo, K., Davis, S., et al
1
Ogle, G.
1
Ogoina, D.
1
ohns Hopkins Center for Communication Programs
1
ois Chappui, F.
1
Ojji, D.B.
1
Okech, U.K.
1
Okoye, CI.
1
Oladapo, O.T
1
Olans R. N. , R. D. Olans, A. DeMaria Jr
1
Oliveira e Souza, R.
1
Oliveras, Laura
1
Olivia Fiertag, Sharon Taylor, Amina Tareen & Elena Garralda
1
Olivia Tiberi
1
Olney, Jack J.
1
Omasete J., Forster J., Geere J., et al.
1
Ombok, C.A., Obondo, A., Kangethe, R. & Atwoli, L.
1
Omidian, P.
1
Omowunmi Aibana , Andrej Slavuckij , Mariya Bachmaha, et al.
1
OMS (WHO)
1
OMS, École de Santé Publique Johns Hopkins Bloomberg
1
OMS, Ministério da Saúde, ADCGO
1
OMS, OPAS
1
OMS, UNICEF. FAO
1
Onalu, C.
1
One Health Commission
1
One Million Community Health Workers Campaign | mPowering Frontline Health Workers
1
One Million Community Worker Campaign
1
One World Trust
1
Onofrey, L.
1
ONUDC
1
Oosterhoff, P. and Wilkinson, A
1
OPAS, IFRC, GOARN, Unicef
1
Open Heart
1
Open Society Foundation
1
Open Society Institute - Public Health Program
1
Open Society Institute International Harm Reduction Development
1
OPHI (Oxford Poverty and Human Development initiative)
1
Ophthalmic Services Unit and the Division of Non Communicable Disease (DNCD), Ministry of Health Kenya
1
OPP-ERA, et al.
1
Oppah Kuguyo, A. Matimba, Nomsa Tsika, et al.
1
OPSIC
1
Optimal Blood Use Project
1
Ordre National des Médecins
1
Organisation de la Santé Mondiale, Bureau Regional de l'Afrique
1
Organisation mondial de la Santé
1
Organisation Mondiale de la Santé
1
Organisation mondiale de Santé
1
Organisation mondiale de la Santé (Amériques )
1
Organisation mondiale de la Santé (Amériques)
1
Organisation mondiale de la Santé (OMS), Bureau régional de l’Afrique
1
organisation mondiale de la Santé (OMS), Fédération internationale pharmaceutique (FIP)
1
Organisation mondiale de la Santé (OMS), Groupe consultatif stratégique et technique sur les maladies tropicales négligées, Groupe de travail du contrôle et de l’évaluation
1
Organisation mondiale de la santé (OMS), Organisation panaméricaine de la santé, Fédération internationale des Sociétés de la Croix-Rouge et du Croissant-Rouge
1
Organisation mondiale de la Santé, Bureau régional de l'Europe
1
Organisation monidale de la Santé OMS
1
Organización Funciones del Insitituto Nacional de Estadística e Informática, Peru
1
Organización Internacional para las Migraciones Misión con Funciones Regionales para el Cono Sur
1
Organización Mundial de la Salud (Las Américas)
1
Organización Mundial de la Salud (OMS), Federación Internacional Farmacéutica (FIP)
1
Organización Mundial de la Salud Américas
1
ORGANIZACIÓN MUNDIAL DE LA SALUD, ORGANIZACIÓN PANAMERICANA DE LA SALUD
1
Organización Mundial de la Salud, War Trauma Foundation, Visión Mundial Internacional.
1
Organización Panamericana de la Salud
1
Organización Panamericana de la Salud PAHO
1
Organización Panamericana de la Salud, Ministerio de la Salud Pública y Bienestar Social, et al.
1
Organización Panamericana de la Salud, Ministerio de la Salud Pública y Bienestar Social, Paraguay et al.
1
Organización Panamericana de la Salud, Ministerio de Salud y Protección Social
1
Organización Panamericana de la Salud, Organización Mundial de la Salud
1
Organización Panamericana de la Salud, Programa Mundial de Alimentos, Fondo de las Naciones Unidas para el Desarrollo del Niño
1
Organizacíon Munidal de la Salud OMS
1
Organização Mundial da Saúde, World Trauma Foundation, World Vision
1
Organização Mundial da Saúde. Escritório Regional para a África
1
Organização Mundial de Saúde
1
Organização Pan-Americana da Saúde
1
Organização Pan-Americana da Saúde e Ministério da Saúde
1
Organizaición Mundial de la Salud (OMS)
1
Oriol Mitjà, M.D., Ph.D., Wendy Houinei, H.E.O., Penias Moses, et al.
1
Orr, B.J., A.L. Cowie
1
Ortiz-Jiménez
1
Osama Abas, Faten Abdelaziem & Ayman Kilany
1
OSF and OSISA the Centre for Human RightsPretoria University Law Press (PULP)
1
Osman, H.
1
Osório, D.V.
1
Ostroff, J.L.
1
Ostroff, M.L.
1
Oswald, S. H., Ernst, C., Goldbeck, L.
1
Ouedraogo Y., Furlane G., Fruhauf T. et al.
1
Ouédraogo M., Samadoulougou S., Rouamba T. et. al.
1
Over M.
1
Overseas Development Institute
1
Overseas Development Institute (ODI)
1
OVID-19 Excess Mortality Collaborators
1
Oxfam Deutschland e.V.
1
Oxford
1
Oxford Academic - International Health
1
Oxford, et al.
1
Oyenuga, V.
1
Ozar, D.T.
1
Ozho, O.B.
1
Ozioko ,KU.
1
Ozoh, O.
1
Ö. Göpınar
1
Öhlmann P.
1
Österreichisches Rotes Kreuz
1
Öztürk, H.
1
O’Connell, Meghan
1
O’Neill, D.W.
1
O’Neill, J.
1
O’Sullivan BG., Chater AB, Bingham A., et al.
1
P. Bakibinga, Kamande E. , Kisia L., et al.
1
P. Bayr
1
P. Ndokweni
1
P. Ngangue
1
P. A. Omungo
1
P. Berry, K. Ebi and L. Varangu
1
P. Booth
1
P. Brouwers
1
P. Brysiewicz and B.R. Bhengu
1
P. Case
1
P. Collignon, J.J.Beggs, T.R. Walsh, et al.
1
P. De Castro
1
P. Delchevalerie
1
P. Drain, and T. Hall
1
P. E. Farmer et al.
1
P. Fernández-Dávila
1
P. Fritsch
1
P. Glaziou, C.Sismanidis, P. J. Dodd, et al.
1
P. I. Fujiwara, R. A. Dlodlo, O. Ferroussier, et. al
1
P. J. Dodd
1
P. K. Jain
1
P. K. Maulik
1
P. Kruger
1
P. Lloyd-Sherlock
1
P. M. Enright, J. Shumake-Guillemot et al.
1
P. M. Kelly
1
P. Monfiston
1
P. Mulongeni
1
P. N. Stearns
1
P. Nyasulu, S. Mogoere, T. Umanah, et al.
1
P. O. Zogo2
1
P. Ozório
1
P. Pereznieto
1
P. Pipero
1
P. T. Fernandes
1
P. Tamony and M. Turner
1
P. Thierry Houngbo, Tjard De Cock Buning, Joske Bunders, Harry L. S. Coleman, Daton Medenou, Laurent Dakpanon†, Marjolein Zweekhorst
1
P. Viiklepp, P. de Colombani, A. Kurbatova, et al.
1
P. Viiklepp, P. de Colombani, A. Kurbatowa, et al.
1
P. Wamala-Mucheri, C. Otterness, et al.
1
P. Zhai
1
P. Zheng
1
P. Zitko, Á. Passi-Solar et al.
1
P. Zucs
1
P. Zucs, et al.
1
P.A. McQuide, R.-L. Kolehmainen-Aitken, N.Forster (Human Resources for Health)
1
P.A.M.Schreuder and B. Naafs
1
P.M. Rodrigues de Souza, B. da Costa Thomé et al.
1
Paccaud, F. et al.
1
Paciaroni, M.
1
Padilla, M.
1
Padrão P
1
Paediatrica Indonesiana
1
Paex I, Cederno J.R., Paredes Arce P. et al.
1
Paget Stanfield, Martin Brueton, Michael Chan, Michael Parkin, and Tony Waterston
1
PAHO Pan American Health Organization
1
PAHO, WHO
1
Pain & Policy Studies Group
1
Paipilla, K., Castro-Arroyave, D., Grajales,L. et al.
1
Pakoyo Fadhiru Kamba, Munanura Edson Ireeta, Sulah Balikuna et al.
1
Palacio, M.G.
1
PALIAMED (Fundación de Medicina Paliativa de El Salvador)
1
Palmero, D.
1
Pan African - Medical Journal
1
Pan American Health Organisation PAHO, et al.
1
Pan American Health Organization PAHO
1
Pan American Health Organization (PAHO
1
Pan American Health Organization (PAHO), World Health Organization - Regional Office for the Americas (WHO)
1
Pan American Health Organization (Regional Office of the World Health Organization)
1
Panafrican Med Jounal
1
PanAfrican Medical Journal
1
Panaveyi Vicky Malou Adom, Edgard Marius Ouendo, Lamidhi Salami, Gado Napo- Koura, Michel Makoutodé
1
Panday, S., P. Bissell , E.van Teijlingen, et al.
1
Pandey, J. P., M.R. Dhakal, S. Karki, P. Poudel, and M.S. Pradhan
1
Pandit-Rajani, T.
1
Pandit-Rajani, T., S. Sharma, and F. Muramutsa.
1
Panel on Antiretroviral Guidelines for Adults and Adolescents
1
Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children
1
Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV
1
Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents
1
Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents.
1
Paniz-Mondolfi, A.E.
1
Paniz-Mondolfi, P.
1
Panko Reis, J.
1
Panorma Perspectives
1
Panteli, E.
1
Pantelias, A.
1
Paola Di Giulio, Dimiter Philipov, and Ina Jaschinski
1
Paolella, D .A.
1
Paone, M.
1
Papadopoulos, E.
1
Paraguay Todos y Todas
1
Parasites & Vectors
1
Pardo, R.
1
Park, J.J.
1
Parker, J.
1
Parks, Will
1
Parliament of Lesotho
1
Parliament of the United Republic of Tanzania
1
Partners In Health
1
Patel V, Simon G, Chowdhary N, Kaaya S, Araya R
1
Patel V.
1
Paterson, J.
1
PATH
1
Pathfinder International
1
Patricia J. Rogers, RMIT University (Australia) and BetterEvaluation
1
Patricia M.C. Huijbers, Carl-Fredrik Flach, D.G. Joakim Larsson
1
Patricio V. Marquez, and Shekhar Saxena
1
Patrick Corrigan
1
Patrick Smith, T. Dalgleish and R. Meiser‐Stedman
1
Patrick Vinck ,Phuong Pham
1
Patrick, S., Perrin, S., Tim, D., Richard, M-S., David M, C., & William, Y.
1
Pattanaik, D.
1
Patuzzi
1
Paudel, D., A. Thapa, P. R. Shedain, and B. Paudel
1
Paudel, D., Shrestha, I.B., Siebeck, M. & Rehfuess, E.A.
1
Paul J. Schramm, Munerah Ahmed, Hannah Siegel, Jamie Donatuto et al.
1
Paul Roddy, Natasha Howard, Maria D. Van Kerkhove, et al.
1
Paul, A., Adeloye, D., George-Carey, et al.
1
Paul, R.E.
1
Paula Hoffmeyer-Zlotnik
1
Pavic, Z.
1
Pazan, F.
1
Páez Silva, Gustavo Alejandro
1
PD Dr. med. M. Backmund
1
Peace Corps
1
Pearce E.
1
Pedrozo e Silva de Azevedo, C.
1
Peer J
1
PeerJ Preprints
1
Peiris, D.
1
Pemerintah Provinsi Papua Dinas Kesehatan
1
Penman, J.
1
People's Health Movement
1
Pepe VLE
1
PEPFAR (U.S. President's Emergency Plan for AIDS Relief), AIDSTAR-One
1
PEPFAR;
1
Peprah Opoku,M.
1
PERC
1
Pereira A.M. , Aranda M. J. et al.
1
Perez Calderon, Luis Jorge
1
Perrotta, Kim
1
Perry, H.
1
persee
1
Pescarini, J. M.
1
Peter Bakker
1
Peter Elyanu
1
Peter G. Smith, Richard H. Morrow, and David A. Ross
1
Peter Johnson
1
Peter N. Stearns
1
Peter Stastny
1
Peter W Luckow, Avi Kenny, Emily White, et al.
1
Petersen, I.
1
Petry, Nicolai and others
1
Peyton, D.
1
Pérez Franco
1
Pfefferbaum, B., Shaw, J.A. & American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI)
1
Pförtner, K.
1
PGP, UNICEF, Yale Institute for Global Health
1
Phafoli, Semakaleng et al.
1
Pharmacient sans Frontières
1
Pharmacopoeia Commission for Indian Medicine & Homoeopathy, Ministry of AYUSH, Government of India
1
Pharmacy Board of Australia
1
Pharmacy Board of Sierra Leone (PBSR)
1
Pharmacy Board Sierra Leone
1
Pharmacy, Medicines & Poisons Board, Malawi
1
Philippine Heart Association
1
Philippine Society for Microbiology and Infectious Diseases, Philippine College of Chest Physicians, Philippine Academy of Family Physicians
1
Philippines, Department of Health, Epidemiology Bureau
1
Philipps,J.A., et al.
1
Phillipa Hay & Jane Morris
1
Phillips, O.
1
Phillips, Tamsin K.
1
Phimemon, Rune N., Michael J. Mahande, and Habib O. Ramadhani
1
Phoenix Australia
1
Physicians for Human Rights (PHR)
1
Piernas C.
1
Pierre André Michaud, Valentina Baltag, Venkatraman Chandra-Mouli et al.
1
Pierre Perrin
1
Pijnenburg, M.W.
1
Pim Cuijpers, Laura Shields-Zeeman, Bethany Hipple Walters, Ionela Petrea
1
Pinder, Étoile
1
PITCH (Partnership to Inspire, Transform and Connect the HIV response)
1
Pitrez, P. M.
1
Pitt C.
1
Pitt1, C.
1
Pittalis, C.
1
Piva P., Dodd. R.
1
Pl:Pulido M.
1
Plavgo, Ilze, Martha Kibur, Mahider Bitew, Tesfayi Gebreselassie, Yumi Matsuda, and Roger Pearson
1
PLOS Global Public Health
1
PLOS Biology
1
PLOS Blogs Lattitude
1
PLoS Global Public Health
1
PLOS journals
1
PLOS ONE, which is part of the Public Library of Science (PLOS)
1
PLOS Phatogens
1
PMC - US National Library of Medicine National Institutes of Health
1
PMC Public Health
1
PMH
1
PNAS
1
Pneumonia
1
PNUD
1
Poe Poe Aung
1
Pohlig G, Bernhard SC, Blum J, Burri C, Mpanya A, et al.
1
Pointifical Council for Justice and Peace
1
Polack, F.P. et al.
1
Polanco-Pasaje JE, Rodríguez-Márquez I, Tello-Hoyos KY et al
1
Polanco-Pasaje, J.E.
1
Pollack L. A., D. Plachouras, H. Gruhler et al.
1
Polly Clayden, Simon Collins, Mike Frick, et al.
1
Pontes LM, Martins CB, Napolitano IC, Fonseca JR, Oliveira GM, Iso SM, Menezes AK, Vizzotto AD, di Sarno ES, Elkis H.
1
Popa G.
1
Population Health Metrics
1
Population Reference Bureau
1
Portaels, F-
1
Portaels, F.
1
Portella, C.
1
Porto, V.
1
Potet, J.
1
Pothuis, Michal et al.
1
Potokra, T.
1
Potter, A.L., Vandy, M., Smart, N. Blanchet, K.l.
1
Powell-Jackson, T.
1
Powers, W.J.
1
Pozzer, A.
1
Pöschl, U. et al.
1
Prabhakaran, D.
1
Practical Action Publishing
1
Pradhan, Y.V., Upreti, S.R., Pratap, K.C.N, et al.
1
Prather, K.A., C.C. Wang , and R.T. Schooley
1
Praveen, D. et al.
1
Preety Das
1
President's Emergency Plan for AIDS Relief
1
President's Malaria Initiative
1
President’s Malaria Initiative
1
President’s Malaria Initiative, CDC, MCHIP, MCSP
1
Preussler, S.
1
Prevent Project
1
Prgramme nationale de la lutte contre le paludisme (Sénégal)
1
Prgramme nationale de lutte Contre la Tuberculose
1
Priebe, S.
1
Prin, M.
1
Prince
1
Priotto, G.
1
Prison Department
1
Prisons Care & Counselling Association
1
Pro health Regio, et al.
1
Proceedings of the Nutrition Society
1
Prof Frank Peters
1
Prof. C. Abobltins, L. Brown, Prof N. Curtis, et al.
1
Prof. Dr. Kurnaz, S.
1
Prof. Dr. med. J.Reimer, MBA
1
Prof. Dr. P. Bendel
1
Prof. G. N. Lule, Dr. B. Nyawira
1
Professor J. Lundgren
1
Progama Nacional de Control de Zoonosis
1
Program for Appropriate Technology in Health PATH
1
Programa Nacional de Controlo da Malária (PNCM)
1
Programa Nacional de Controlo da Malária (PNCM), Organização Mundial de Saúde (OMS)
1
Programme Evaluation Organisation, Planning Commission, Government of India
1
Programme national de lutte contre le paludisme (PNLP) - Sénégal
1
Programme National de lutte contre la Tuberculose (PNT) - Sénégal
1
Programme national de lutte contre la tuberculose - Sénégal
1
Programme National de Lutte Contre le Paludisme - Sénégal
1
Programme national de lutte contre le paludisme (PNLP) - Sénégal
1
Programme National de Lutte contre le sida, Le Ministère de la Santé Publique de Madagascar
1
Programme National de Lutte contre les IST
1
Programme National de Nutrition (PRONANUT)
1
Programme National Multisectoriel de Lutte contre le Sida (PNMLS), RD Congo
1
Programme National Multisectoriel de Lutte contre le VIH
1
Programme nationale de lutte contre le plaudisme (PNLP) - Sénégal
1
Programme Spécial de Recherche et de Formation concernant les Maladies Tropicales (TDR), Organisation mondiale de la Santé
1
Promotion Santé Suisse
1
PROMUNDO-US, UNFPA
1
ProQuest Dissertations & Theses
1
Prosad
1
Protection Cluster, UNFPA
1
PROVEA , Programa Venezolano de Educación - Acción en Derechos Humanos
1
Provinske P.
1
Pruess, A.
1
Prüss-Ustün A., Wolf J., Bartram J., et al.
1
Prüss-Ustün, A.
1
Prykhodko, I.I.
1
Prynn, J.E.
1
Pryor, W.
1
PSA Tansforming The Supply Chain
1
Psychosocial Centre
1
Psychosoziales Zentrum für Flüchtlinge Düsseldorf
1
PtoP (From Protection to Protection)
1
Public Health Association of South Africa (PHASA)
1
Public Health Foundation India
1
Public Health Reviews
1
Public Library of Science PLOS
1
Publicación de las Naciones Unidas
1
Publications Office
1
Publisher: National Academic Press
1
Pudjiastuti, P., A. Rodjani, L.K. Wahyuni, et al.,
1
Puerto Castro GM, Montes Zuluaga FN, Alcalde-Rabanal JE, Pérez F, et al.
1
PUPH, Université Lyon1 (ISPB-Faculté de Pharmacie) et Hospices Civils de Lyon
1
Purcell, L
1
Purgato, M., Gross, A.L., Betancourt, T., et al
1
Putica, B.
1
Qreini, M.
1
Quatar Foundation
1
Queensland Government
1
Quiggin D., et al.
1
Quintero X.G.
1
Quirk, E.J.
1
R Sari Kovats et al.
1
R Wood, L-G. Bekker
1
R. and Coimbra Brito
1
R. A. Golin
1
R. Ahmad, S.Shahzad Hasan, et al.
1
R. Barnabas
1
R. Bieri, S.S. Thomas, et al.
1
R. Bucciardini
1
R. Cañizares Fuentes,J. Cuenca Vega et al.
1
R. Coker
1
R. Colebunders, A. Hendy, J.L. Mokili, et al.
1
R. D. Costa Benavides, V. C. Altamirano, A. L. Alvarado et al.
1
R. D. Harrington
1
R. Diel, A. Nienhaus
1
R. Diel, B. Hauer, R. Loddenkemper, et al.
1
R. Doshi
1
R. Dunbar
1
R. E. Dew, H.G. Koenig, et al.
1
R. E. Verin
1
R. Elovich
1
R. Felix
1
R. Furth
1
R. G. Ponce de Leon
1
R. G. Thomas-Reilly, F. Tozija, V. Soltan
1
R. Gaßmann
1
R. Gustav
1
R. H. Remien
1
R. Heimer
1
R. Jahn
1
R. James
1
R. Jenkins
1
R. Kidd
1
R. Knottneruset al.
1
R. Kronick
1
R. Lessells, K. Mlisana and T. de Oliveira
1
R. Leyva-Flores
1
R. M. David
1
R. Martín-Cañavate
1
R. Muloiwa
1
R. Nefdt, E. Ribaira and K. Diallo
1
R. Pebody
1
R. Pendse
1
R. R. Althoff
1
R. S. Diler
1
R. S. Fisher
1
R. S. Mastrorosa, M. Conceição do Rosário
1
R. Shenoy, M. Das, H. Mansoor, et al.
1
R. Smart
1
R. Thapar
1
R. Thompson, G. Fontana, et al.
1
R. Turner
1
R. Velayudhan
1
R. Walker
1
R. White
1
R.A. Fowler, N.K. Adhikari, et al.
1
R.Beaglehole, and T. Kjellström
1
R.d M. Rapee
1
R.D. Alarcón & S.A. Aguilar-Gaxiola
1
R.G. Wagner, I. Petersen, et al.
1
R.H. Dios, et al
1
R.l Kronick
1
R.M.
1
R.M. de Oliveira Costa et al.
1
R4V
1
Raafat, N.
1
rabhakaran, Dorairaj
1
RACGP
1
Rachel Phillipson
1
Radcliffe
1
Radiation Emergency Medical Management (REMM)
1
Raditladi, Tirelo et al.
1
Raftery A, Tudor C, True L, Navarro C
1
RAG. Khammissa, R. Ballyram, et al.
1
Rahardjo, H.E., B.I. Santoso, S. Hakim, et al.,
1
Rahman-Shepherd, A.
1
Rahmat, R.
1
Rahul Shidhaye
1
Rajagopal, D.
1
Rajagopalan, S.
1
Rajan, S.
1
Rajat Khosla, Moazzam Ali and Jane Cottingham
1
Rajbongshi, S.
1
Rajesh Upadhyay, Milind Y Nadkar, A Muruganathan
1
Rajiha A. Ibrahim, Amete M. Teshal, Surafel F. Dinku, et al.
1
Ralf Krumkamp, Sandra Mounier-Jack, Amena Ahmad, Ralf Reintjes, Richard Coker
1
Ramaiah, K. D.
1
Ramanathan, K.
1
Ramasamy, Selvaraju
1
Ramcharitra Shah
1
Ramsey,J.
1
Ramukumba, M.M.
1
Rana Y.
1
Ranaweera, S.
1
Randers, J.
1
Rangarajan, S. et al.
1
Ranjita Misra
1
Rao, S.P.S.
1
Rashan, S.
1
Rashan, S. et al.
1
Rasmussen, D.J., Karsberg, S., Karstoft, K-I. & Elklit, A.
1
Rassi A., Dias J.C.P., Marin-Neto J.a.
1
Ravi Narayan and Unnikrishnan PV
1
Ravindranath R Tongaonkar, David L Sanders and Andrew N Kingsnorth
1
Ravinetto, R. et al.
1
Ray, K.K.
1
Razum, O., V. Penning, A. Mohsenpour, et al.
1
Râjnoveanu, R.M.
1
rbfhealth.org
1
RCC Service
1
RCCE Collective Service
1
ReAct Action on Antibiotic Resistance
1
Rebecca Esliker, University of Makeni
1
Rebecca Holmes
1
Rebuilding Basic Health Services Project (RBHS)
1
Red Cross Red Crescent Climate Centre
1
Red Nacional por los Derechos de las Personas Travesti, Transgénero y Transexuales del Perú
1
Redfern, J. et al.
1
Rediscovering Biology
1
RedR UK
1
Redvers, N.
1
Reed, Brian | Shaw, Rod
1
Rees, D.
1
Rees, E.M.
1
Refugee Guide Online
1
Refugee Studies Centre, UK
1
Refugee Studies Centre, University of Oxford
1
Refugee Study Centre
1
Refugees International (RI)
1
refugio stuttgart e.v.
1
Regan A., Thompson G.
1
Regina Hiller
1
Reginald A. Annan, Patrick Webb, Rebecca Brown
1
Regionaalhaigla
1
Regional Office Europe
1
Registered Nurses Association (RNAO)
1
Regula Buchli
1
Rehabilitation Council of India, Ministry of Social Justice and Empowerment
1
Rehabilitation Division
1
Reid, G.
1
Reijer, P.
1
Reilly, K.
1
Reith, G.
1
Reliefweb OCHA
1
Religions
1
Remans, R.
1
REMM, RITN
1
Remnant, J.
1
Ren, F.
1
Renner B.
1
Rentschler, J.
1
REPOA
1
Repoductive Health Journal
1
Reproductive and Child Health Directorate
1
Reproductive Health Division Community Health Department Ministry of Health Uganda
1
Reproductive Health Matters
1
Reproductive Health Response in Conflict Consortium
1
Republic of Ghana
1
Republic of Kenya
1
Republic of Kenya Ministry of Health
1
Republic of Lebanon, Ministry of Health
1
Republic of Libera, Ministry for Health and Social Welfare
1
Republic of Liberia
1
Republic of Liberia, Ministry of Health and Social Welfare
1
Republic of Rwanda
1
Republic of Sierra Leone, Ministry of Health and Sanitation
1
Republique Democratique du Congo , Ministère de la Santé, Secrétariat General à la Santé
1
Republique Democratique Du Congo Ministere de la sante Programme National de Lutte Contre le SIDA et les IST
1
Republique du Sénégal, Ministère de la Santé
1
RESAOLAB Guinée
1
Research
1
Research and reports in tropical medicine
1
Research Institute for Tropical Medicine National Tuberculosis Reference Laboratory
1
Research Square
1
ResearchGate.net
1
Resende, M. B.
1
Resnikoff, S.
1
Respiratory Medicine
1
Respiratory Medicine (2005) 99, 553–558
1
Respiratory Medicine (2006) 100, 616–621
1
Respiratory Research
1
Restless Development
1
Reusken C. B. E. M., E. K. Broberg, B. Haagmans et al.
1
Rev Neuropsiquiatr
1
Rev Panam de Salud Pública
1
Rev. Gerenc. Polit. Salud, Bogotá, Colombia
1
Review on Antimicrobial Resistance
1
Revista Brasileira de Geriatria e Gerontologia
1
Revista Brasileira de Psiquiatria
1
Revista Cientifica FMC
1
Revista de Psicología Clínica con Niños y Adolescentes (RPCNA)
1
Revista de Saúde Pública
1
Revista Latinoamericana de Desarrollo Económico
1
Revista Medica Uruguay
1
Revista médica de Chile
1
Revue canadienne de soins infirmiers en oncologie
1
République de Guinée - Ministère de la santé
1
République Démocratique du Congo
1
République Démocratique du Congo, Ministere de la Sante, Programme national de lutte contre le SIDA & IST (PNLS)
1
République Démocratique du Congo, Ministère de la Santé
1
République Démocratique du Congo, Ministère de la Santé Publique
1
République Démocratique du Congo, Ministère de la Santé Publique, Programme National de la Lutte contre le Paludisme (PNLP)
1
République Démocratique du Congo, Province du Kwilu
1
République du Bénin
1
République du Bénin Ministère de la Santé Direction de la Santé de la Mère et de l’Enfan
1
République du Cameroon
1
République togolaise, Ministère de la Santé et de la Protection Sociale
1
République togolaise, Ministère de la Planification, du Développement et de l’Aménagement du Territoire, Ministère de la santé
1
République Tunienne - Ministére de la santé
1
Réseau africain pour les soins aux enfants affectés par le sida (ANECCA)
1
Rhee, J.Y.
1
Rhodes, T.
1
Ricardo Heinzelmann, Rogerio Luz Coelho Neto et al.
1
Richard Vergunst, Leslie Swartz, Gubela Mji, Malcolm MacLachlan & Hasheem Mannan
1
Richards, P.
1
Richardson, C.R.
1
Richardson, M.P., Chadwick, D.W. & Wehner, T.
1
Riggirozzi P., J. Grugel, N. Cintra
1
Right to Care (Training Health Seriously)
1
Ringwald, J. et al.
1
Rippon, S.
1
Ritu Kalgotra, Jaspal Singh Warwal
1
Roberson, L. et al.
1
Robert A. Scott, Samden D. Lhatoo & Josemir W.A.S. Sander
1
Robert E. Black, Ramanan Laxminarayan, Marleen Temmerman
1
Robert Koch Institut - RKI
1
Robert Koch Institut RKI
1
Robert-Koch-Instiut RKI
1
Roberto Chaskel, James M. Shultz, Silvia L. Gaviria, et al.
1
Roberto Dullak, Monica Ruoti, et al.
1
Roberton, T.
1
Roberts B.
1
Robertson A., Malan A., Greenfield D.
1
Robin G. and J. Balbus
1
Rocha, R.
1
Rochweg, B.
1
Rodrigues da Silva, M.
1
Rodrigues R., S. Ilinca, K. Schulmann
1
Rodriguez, A.
1
Rodriguez-Morales, A. J. and Franco O. H.
1
Rodríguez-Márquez I. , Tello-Hoyos K. Y., et al.
1
Rodríguez-Muñoz, M. F., Krupelnytska, L. et al.
1
Rodríguz-Alonso, B.
1
Rohleder, S.
1
RohrI, J.R.
1
Rohwerder, B.
1
Roja-Palma, C.
1
Rojas, C. L., Polanco E. C., Vivar M. C. et al.
1
Rojas-Rueda, D.
1
Roma Active Albania
1
Romanello M., McGushin A., et al.
1
Romanello M., van Daalen K., et al.
1
Romanian Angel Appeal
1
Román-Rodríguez, M.
1
Rongbin Xu, Qi Zhao, M.S.Z.S. Coelho et al.
1
Rontgene M. Solante, Manolito L. Chua
1
Roos N.
1
Rosas, F.
1
Roschnik S.
1
Rosenbaum, Julia and Bery, Renuka
1
Rosengren, A.
1
Ross-Degnan, D., Vialle-Valentin, C., and Briggs, J.
1
Rostal, M.K.
1
Roullaud, S.
1
Rousham E. K., M. Aminul Islam, P. Nahar et al.
1
Routledge (Taylor & Francis Group)
1
Rouw, A.
1
Roy, S. et al.
1
Royal Australian College of General Practitioner
1
Royal College of Obstetricians and Gynaecologists
1
Royal College of Paediatrics and Child Health
1
Royal College of Psychiatrists
1
Royal Netherlands Academy of Arts and Sciences
1
Royal Pharmaceutical Society, etal.
1
Royal Society open Science
1
Röbbel, N.
1
Röhrs S, Delany A & Mathews S
1
Rubaihayo, J., N.M. Tumwesigye, J. Konde-Lule, et al.
1
Rubiano-Mesa Y. L. , Saavedra-Cantor C. J.
1
Rubinstein, F.
1
Rubinyi, S.
1
Rude, B.
1
Ruder, S.
1
Ruff, P.
1
Rugigana, Etienne, Francine Birungi, and Manassé Nzayirambaho
1
Rumunu, J. et al.
1
Rune J. Simeonsson
1
Rupérez et al.
1
Rupprecht, C.
1
Rusakaniko, S.
1
Ruth Naylor
1
Rutstein, S.E., J. Ananworanich, S. Fidler, et al.
1
Rüppel T., Rüppel J.
1
Rwanda Biomedical Center, National Reference Laboratory Division
1
Rwanda Medical Journal / Revue Médicale Rwandaise
1
Ryan, D.
1
Ryan, R.E.
1
Rylance, S.
1
Røttingen, J.A.
1
S .Gulati
1
S Karthick and Sangita Barwa
1
S. Lam, Nguyen H. T. T., Tuan H. N. H., et al.
1
S. A. Madhi
1
S. A. Roberts et al.
1
S. Ali, A. Haileamlak, A. Wieser, et al.
1
S. Andersson, A. Heaton, et al.
1
S. Asfaw
1
S. Assegid
1
S. Basu
1
S. Bernays
1
S. Bhattachrya
1
S. Brusamento
1
S. Brünink
1
S. Buchan
1
S. Buda
1
S. C. Cavalcante
1
S. Cabrera
1
S. Chakraborty, K. Syal, R. Bhattacharyya, et al.
1
S. Chauwa Phiri, M.Lippitt Prust, C. Phiri Chibawe, et al.
1
S. Chen
1
S. Chynoweth, D. Quick et al.
1
S. Clay
1
S. Colt, M.N. Garcia-Casal, J.P. Peña-Rosas, et al.
1
S. Custer
1
S. D. Blacksell and R.J. Maude
1
S. D. Owolabi
1
S. Dagron
1
S. de Bruin, J. Knoop and J. van Vliet
1
S. Dilmitis
1
S. E. Kellerman
1
S. E. Krauss
1
S. E. Mellors
1
S. Ebrahim
1
S. F.Jakobsen
1
S. Ferreira Júnior, H. B. de Oliveira, L. Marin-Léon
1
S. Ferron and M. O'Reilly
1
S. Galwankar
1
S. Gies
1
S. Gogochashvili
1
S. Groth, G. Forte et al.
1
S. H. E. Kaufmann, T. G. Evans, W. A. Hanekom
1
S. H.-L. Fry
1
S. Harvest, C. Litzke, P. Akil, et al.
1
S. Hatherill
1
S. Hermans
1
S. Hung
1
S. I. Ngulde
1
S. Ijaz
1
S. Juneja
1
S. K. Das
1
S. K. Dlamini
1
S. Kaba
1
S. Khazei
1
S. Kolmes
1
S. Kromann Jensen
1
S. Kwon et al.
1
S. L. Asangbeh, et.al.
1
S. L. Barnabas
1
S. Ladhani
1
S. Lahri, and D.J. van Hoving
1
S. Laver
1
S. Lazzari and G. Kiesner
1
S. Le Coeur
1
S. Lee
1
S. Lees et al.
1
S. Lordemus
1
S. M. Essajee
1
S. M. Kibusi
1
S. M. Nsagha
1
S. Mahroof-Shaffi, C. Harkensee, A.T Chamberlain
1
S. Mc Coy, D. Ngilanwa, et al.
1
S. McLean
1
S. Meshnick, M. Janko, S. Doctor, et al.
1
S. Mishra
1
S. Mitra
1
S. Mokitimi
1
S. N. Naicker
1
S. Nachman et al.
1
S. Nyaude
1
S. Oza, A.A. Sesay, N.J. Russel, et al.
1
S. P. Saha
1
S. Palitz
1
S. Phanouvong, C. Raymond, L. Krech, Y. Dijiba, B. Mam, P. Lukulay, D. Socheat, T. Sovannarith and C. Sokhan
1
S. Rahman Mashreky, et al.
1
S. Rezaeian
1
S. Ripoll and S. Carter
1
S. Rohleder, M. Qreini, et al.
1
S. Rueda
1
S. Sarkar
1
S. Saxena
1
S. Song
1
S. Stash
1
S. Stefanello
1
S. Sweeney
1
S. Uysal
1
S. Vorkorper
1
S. Warren
1
S. Woodgate
1
S.B. Calderwood and A.Bloom
1
S.Dvoriak
1
S.Kinloch-de Loës, et al.
1
S.M Kariuki, S. M Kinyanjui, et al
1
S.Mabunda
1
S.Noto
1
S.R. Lewin and R. Sherer
1
S.Taylor
1
SAARC Tuberculosis and HIV
1
Saarnak, C.
1
SAATHII (Solidarity and Action Against The HIV Infection in India)
1
Sabiha Essack
1
Sachs, J.
1
Sachs, J. D.
1
Sachs, J., Karim, S., Aknin, L. et al.
1
Sachverständigenrat für Migration und Integration
1
Sachy, M
1
Sacks, E.
1
Sadat, N. et al.
1
SADC
1
SADJ
1
Sadoff,J. and G. Alter
1
Saeboenes, A.-M.
1
Safe Work Australia
1
SAFOD RESEARCH PROGRAMME (SRP)
1
Safrani, N.
1
SAGE Open Medicine
1
SAHARA J.: Journal of Social Aspects of HIV/AIDS
1
SAHARA-J: Journal of Social Aspects of HIV/AIDS
1
SAHRC
1
Sai Sam Hkam
1
Saiful Islam M. , Mizanur Rahman K., Sun Y., et al.
1
Saimiento, Juan Pablo et al.
1
Saint-Pere Francois
1
Saint-Pierre Francois
1
Salehi, M.
1
Salud Entre Culturas
1
Salvage J, Rowson M, Melf K and Sandøy I
1
Salvage J, Rowson M, Melf K, Wilmen A
1
Salvatore Noto, Pieter A. Schreuder and Bernard Naafs
1
Salvi, S.S.
1
Samalin, L.
1
SAMHSA’s Trauma and Justice Strategic Initiative
1
SAMJ
1
SAMJ Research
1
Samson, A.
1
San Pedro Francisco
1
San Román, N. C., et al
1
Sana-Al-Sukhun, C. Blanchard, et al.
1
Sandra F. Moreira-Silva1,3, Eliana Zandonade
1
Sandra Kong
1
Sangeeta Raja and Nadeem Mohammad
1
Sanmatino, M.
1
Sanni Yaya , Olalekan A. Uthman, Agbessi Amouzou, Michael Ekholuenetale, Ghose Bishwajit
1
Sanni-Adeniyi, O. et al.
1
Sanson, A.
1
Santero, M.
1
Santesso, N.
1
Santibañez, S., V. Spiegel, M. O'Sullivan, et al
1
Santos, D.
1
Santos-D'Amorim K, Fernandes de Oliveira Mirand MK
1
Santoso, A., A. Rodjani, Tjahjodjati, et al.,
1
Sao Paulo Medical Journal
1
Saouadogo H., M. Compaore
1
Saposnik, G.
1
Sara McLean
1
Sara Pantuliano
1
Saraf, P.
1
Sarah Frost, Chapal Khasnabis, Kylie Mines, and Lourdes de la Peza
1
Saranya A, Selvaraj E Lee, Mason Harrell, et al.
1
Sarity Dodson, Suvajee Good and Richard Osborne
1
Sarkar A, Mburu G, Shukla S, Behara J, et al.
1
Sarr, M.
1
Sarr, M., M. Ba, B. Camara et. al.
1
Sascha Marchang, Natasha Hurley
1
Sasser S,Varghese M, Kellermann A, Lormand JD.
1
Satomi, E.
1
Saudi Journal of Biological Sciences
1
Sauerbrey, M.
1
Saul, R. and D. Philipps
1
Sausgruber, R.
1
Saúde mental, relações raciais e Covid - 19
1
Save the Children (UK) South Africa Programme
1
Save the Children Sweden
1
Save The Children UK
1
Save the Children, Terre des Hommes
1
Saxena, S.
1
Sánchez Báez E.A., Diego D. et al.
1
Sánchez Sánchez, Y.
1
Sánchez-Pérez, H. J.
1
Schafer, A.
1
Schatz, M.
1
Schäferhoff M.
1
Schäferhoff M. et al.
1
Scheeringa, M.S., Amaya-Jackson, L. & Cohen, J.
1
Schell, C.O.
1
Scherr, N.
1
Schieffelin, JS.
1
Schizophrenia Research and Treatment
1
Schmid B, Thomas E, Olivier J and Cochrane JR.
1
Schmid, Stephanie
1
Schmidt, B. et al.
1
Schmidt-Sane M.
1
Schneider, A. et al.
1
Schneider, M.
1
Schneider, M.T.
1
School Health Integrated Programming (SHIP)
1
School of Economics, University of Nairobi
1
Schopler E, Reichler RJ, DeVellis RF et al. Перевод и адаптация Морозова Т.Ю., Довбня С.В.,
1
Schopler E, Reichler RJ, DeVellis RF, Daly K. et al.
1
Schouten, E. et al.
1
Schrade, C.
1
Schramm, P,J.
1
Schraufnagel, D.E.
1
Schröder, H.
1
Schubert L.
1
Schuyler W Henderson, Andrés Martin et al.
1
Schütt, K. et al.
1
Schwalm, J.
1
Schwartz, L.
1
Schwienhorst, E.M.
1
SCIELO
1
Science Publishing Group
1
SCIENCEDOMAIN international
1
Sciences, A.
1
Scientific and Cultural Organization
1
Scientific Committee on AIDS and STI
1
Scientific Cooperation Center "Interactive plus"
1
Scientific Data
1
Scientific Electronic Library Online SciELO
1
Scientific reports
1
SCK-CEN
1
Scott F. Dowell, James J. Sejvar, Lul Riek, et al.
1
Scott S.
1
Scott, C.
1
Searle, L.
1
Sebayang, Susy K., Ferry Efendi, and Erni Astutik
1
Sebit, W.
1
Secretaria de Atencao Primaria Saude (SAPS)
1
Secretaria de estado de Saud de Minas Gerais, Brasil
1
Secretaria de Estado dos Direitos da Pessoa com Deficiência de São Paulo
1
Secretaria de Vigilância em Saúde − Ministério da Saúde
1
Secretaria Extraordinária de Enfrentamento à COVID-19, Brasil
1
Secretaria Municipal de Saúde do Rio de Janeiro
1
Secretaria Nacional por los Derechos Humanos de las Personas con Discapacidad (SENADIS)
1
Secretariat of the Council of Europe Convention on the Protection of Childr en against Sex al Exploitation and Sexual Abuse (Lanzarote Convention)
1
SECTION27
1
SECTION27 - Catalysts for Social Justice
1
Sedas A. C., M. Aguerrebere, L. A. Martinez Juarez, et al.
1
Sedeto M H
1
Segvia, E. V. L. et al.
1
Seitio-Kgokgwe, Gauld, Hill et al
1
Seixas, J.
1
Sekamatte, M.
1
Selma Azabagic, Razija Spahic, Nurka Pranjic, and Maida Mulic
1
Semmes, Oliver John
1
Sena, L.
1
Sentinel Project
1
Seputra, K.P., Tarmono, B.S. Noegroho, et al.,
1
Sequeira, M.D.
1
Sequera V.G., Tostmann A., et al.
1
Serebrisky, D.
1
Serge Ade, Omer Adjibodé, Prudence Wachinou, Narcisse Toundoh, Bérénice Awanou, Gildas Agodokpessi, Dissou Affolabi, Gabriel Adè, Anthony D. Harries, Séverin Anagonou
1
Serge Ade1, Arnaud Trébucq, Anthony D. Harries, Gabriel Ade, Gildas Agodokpessi, Prudence Wachinou, Dissou Affolabi, Sévérin Anagonou
1
Serneels, P. & Lievens, T.
1
Serneels, P., Montalvo, J.G., Pettersson, G., et al.
1
Serrano, C.R. and A.Amarillo
1
Servizio Sanitario Regionale Emilia-Romagna
1
Sessay, S.
1
Seth Mnookin
1
Sethi, T.
1
Setzer Verlag
1
Seung Hee Lee-Kwan, et al.
1
Sexton, S.
1
Sexual and Reproductive Health Matters (SRHM)
1
Sexual Health and Blood Borne Virus Unit Centre for Disease Control
1
Série Informação para ação na Covid-19 | Fiocruz
1
Séverin, T.
1
Séverin, T. et al.
1
SFU MPH Capstone Project
1
Shanaya Rathod, Narsimha Pinninti, Muhammed Irfan, et al.
1
Shaping Health Programme
1
Sharafi, L. et al.
1
Sharifa Begum, et al.
1
Sharma, G. & Pandey, S.R.
1
Sharon Abramowitz, Kristen McLean, Josephine Monger, Kodjo Tehoungue, Sarah McKune, Mosoka Fallah, Patricia Omidian
1
Sharon Alane Abramowitz, et al.
1
Sharon Salmon, Mary-Louise McLaws, Dale Fisher
1
Shaw M.
1
Shaw, A.
1
Shazly Savahl, Sabirah Adams, Serena Isaacs, et al.
1
Shea, DA
1
Shears, Paul, T.J.D. O'Dempsey
1
Sheena Posey Norris, Erin Hammers Forstag, and Bruce M. Altevogt
1
Sheffali Gulati , Jaya Shankar Kaushik, Lokesh Saini, et al.
1
Sheikh, Nurnabi
1
Sheila Leatherman, Somen Saha, Marcia Metcalfe, Dileep Mavalankar
1
Sheila Leatherman, Somen Saha, Marcia Metcalfe, et al.
1
Sheila Nainan Myatra, Naveen Salins, Shivakumar Iyer, et al.
1
Shekhar Saxena , Etienne Krug, Oleg Chestnov et al.
1
Shekhar Saxena and Preston J. Garri
1
Shelah S. Bloom and Svetlana Negroustoueva
1
Shi, W.
1
Shiferaw Dechasa Demissie, et al.
1
Shilpa Ross et al.
1
Shin, D.W. et al.
1
Shire, S.
1
Shiv Gautam, Akhilesh Jain, Manaswi Gautam, et al.
1
Shi‑Lin Chen
1
Shoaib Fahad Hussai, Peter Boyle, Preeti Patel and Richard Sullivan
1
Shotton J.
1
Shrimpton R., Atwood S.
1
Shumbusho, F., van Griensven, J., Lowrance, D., Turate, I., Weaver, M.A., et al.
1
Shyirambere Blaise
1
Sibanda, E.N.
1
Sibanda, E.N. et al.
1
Sibanda-Mulder, Flora
1
SickKids
1
Sida
1
Siddharthan, T.
1
Sierra Leone Red Cross Society
1
Siersma, V.
1
Sightsavers, Department for International Development, The International Trachoma Initiative , et al.
1
Sigmund Freud Privatuniversität
1
Sigridur B.Thormar
1
Sikora, R.A.
1
Silas, Joel
1
Silink, M.
1
Silk Road Studies Program
1
Silva G, Perez F y Marín D
1
Silva, R.
1
Silva, R.R., Alpert, M., Munoz, D.M., Singh, S., Matzner, F. & Dummit, S.
1
Silva, S.
1
Silva-Matos, C
1
Silverman, M.
1
Silvia Dallatomasina, et al.
1
Simate Smate and Yvonne Zimba
1
Simona, Simona J., Mazuba Muchindu, and Harriet Ntalasha
1
Sin, D.D.
1
Singh, A. K.
1
Singh-Phulgenda, S., Dahal, P., Ngu, R. et al.
1
SINTEF Health Research
1
SINTEF Technology and Society Global Health and Welfare
1
Sipsma, H.L., Curry, L.A., Kakoma, J.P., Linnander, E.L., & Bradley, E.H.
1
Sirinivas, S.
1
Siswanto, B.B., N. Hersunarti, Erwinanto, et al.,
1
Slama, S.
1
Sliwa, K.
1
Smith, E.E.
1
Smith, E.M.
1
Smith, J.
1
Smith, J.R.
1
Smyth, A.
1
Snider, L.
1
Social Justice Secretariat
1
Social Science in Humanitarian Action Platform
1
Sociedad Argentina de Pediatría
1
Sociedad Boliviana de Medicina Crítica y Terapia Intensiva
1
Sociedad Boliviana de Medicina Crítica y Terapia Intensiva/ Ministerio de Salud Bolivia
1
Sociedad Boliviana de Obstetricia y Ginecología
1
Sociedad Colombiana de Cardiología y cirugía cardiovascular
1
Sociedad ecuatoriana de geriatria y gerontologia
1
Sociedad Paraguaya de Infectologia (SPI)
1
Sociedad Paraguaya de Pediatria
1
Sociedad Venezolana de Infectología, et al.
1
Sociedade Brasileira de Medicina de Família e Comunidade
1
Sociedade Brasileira de Pneumologia e Tisiologia
1
Societé francaise d'anesthésie et de réanimation (SFAR)
1
Societé francaise d'anesthésie et de réanimation SFAR
1
Society for Gastroenterology Nurses and Associates
1
Society for Maternal-Fetal Medicine (SMFM) Publications Committee
1
Society of Hospital Medicine
1
Socieux
1
SociologieS
1
Soenarta, A.A., Erwinanto, A.S.S. Mumpuni, et al.,
1
Soka, M.J.
1
Soltani A, Ardalan A, Darvishi Boloorani A, et al.
1
Solthis, et al.
1
Sombié I., D. Amendah, K. A. Soubeiga
1
Sonja A. Rasmussen, M.D., Denise J. Jamieson, M.D., M.P.H., Margaret A. Honein, Ph.D., M.P.H., and Lyle R. Petersen, M.D., M.P.H.
1
Sophia University Institute
1
Soriano, J.B.
1
Sorkin, J., Chaney, G., Garcia, M.,et al.
1
Sorkness, C. A.
1
Soucat A.
1
Soumitra Pathare, Michelle Funk, Melvyn Freeman et al.
1
Soumitra Pathare, Руби Холл, Michelle Funk et al.
1
south
1
South Africa Med. J.
1
South Africa's Dept. of Health
1
SOUTH AFRICAN ANTIBIOTIC STEWARDSHIP PROGRAMME (SAASP)
1
South African Centre for Epidemiological Modelling and Analysis (SACEMA)
1
South African Journal of Psychology
1
South African Journal of Psychiatry
1
South African Malaria Elimination Committee (SAMC)
1
South African Medical Journal
1
South African Medical Journal (SAMJ)
1
South African Medical Journey SAMJ
1
South African Nursing Council
1
South Asia Democratic Forum
1
Southeast asian J trop med public health
1
Southern African HIV Cinicans Society
1
Southern African Journal of Anaesthesia and Analgesia
1
Southern African Journal of HIV Medicine
1
Southern African Journal of Infectious Diseases
1
Southern Med Review
1
Souto Medeiros, D. et al.
1
Souza Salles, T.
1
Souza, P.C.A.
1
Spearman, CWN
1
Speier, A.H.
1
Sphere
1
Sphere - Standards
1
SPI
1
Spigel, Lauren
1
Spotlight NSP
1
SPRING - Strengthening Partnerships, Results and Innovations in Nutrition Globally
1
Spring Nutrition
1
Springer Medizin Verlag GmbH
1
Springer Science+Business Media
1
Spudich, S.S.
1
Sri Lanka Journal of Child Health
1
Srinivasan Venkatesan
1
Ssewanyana, D.
1
SSHAP
1
SSOAR
1
SSRC
1
St. George's University of London
1
St. Thomas University
1
STAKOB
1
Standing committee on Nutrition SCN, et al.
1
Standleya C. J., Carlinb E. P., Sorrella E. M. et al.
1
Staples JE, Dziuban EJ, Fischer M, et al
1
State Goverment Victoria
1
State Mental Health Center
1
State of Libya
1
Statistics Division Economic and Social Commission for Asia Pacific Region
1
Steekelenburg, E. V. et al.
1
Steele, Andre
1
Stefan Mauss, et al.
1
Stefan Mauss, Thomas Berg, Jürgen Rockstroh et al.
1
Steffen, W., Noone, K., et al.
1
Stein F, Perry M, Banda G, et al.
1
Stein, L.
1
Steingrüber, S.
1
Stellenbosch University, U.S. Centers for Disease Control and Prevention, and United States Agency for International Development
1
Stender, Stacie
1
Stephen Graham, Malgosia Grzemska, Suzanne Hill et al
1
Stephen J.McPhee
1
Stephen N. Wong, Jane R. Campos, Ian Homer Y. Cua et al.
1
Stephen Sheppard, Richard Hill
1
Stephens, J.W.
1
STEPS Centre, Institute of Development Studies
1
Steve Aldrich, et al.
1
Steve Broach, Luke Clements and Janet Read
1
Steve Peat
1
Stevens, Gretchen
1
Stewart C.
1
Stewart H.
1
Stockholm Reslience Centre
1
Stoddard, Abby
1
Stoknes, P. E.
1
Stolbrink, M.
1
STOP AIDS
1
Stop TB
1
Stop TB Partnership to reach
1
Stop TB Partnership, World Health Organization
1
Stop TB Partnership. Working Group on TB
1
Stork J.
1
Stover J.
1
Straff, W.
1
Strange, A.
1
Strange, A. M.
1
Strautmann, M.
1
Strba Idarraga, L., Alarcón Soto, J.
1
Strengthening Pharmaceutical Systems
1
Strengthening Pharmaceutical Systems (SPS) Program
1
Strengthening South Africa's Response to HIV and Health (SARRAH)
1
Strippoli, M-P. F. et al.
1
STUK
1
SUAHAARA project
1
Suárez, C., Nolder, D., García-Mingo, A. et al.
1
Suárez, V.
1
Suárez-Rozo LF, Puerto-García S, Rodríguez-Moreno LM, Ramírez-Moreno
1
Subho Chakrabarti
1
SUBPAV, SMS-Rio
1
Subsecretaria de Saúde Gerência de Informações Estratégicas em Saúde CONECTA-SUS
1
Substance Abuse and Mental Health Services Administration SAMHASA
1
Suchona Foundation
1
Sudhir Anand and Victoria Fan
1
Sue George, John Dada, Kolawole Maxwell et al.
1
Suliman, S., Kaminer, D., Seedat, S. & Steinm D.J.
1
Sultana, Marufa et al.
1
Sumner,A.
1
Sun, B-X.
1
Sundalic, A. Strossmayer J.J: et al.
1
Sundar, S.
1
Sundewall, J.
1
Sunil Deepak, Franesca Ortali, Geraldine Mason Halls, Tulgamaa Damdinsuren, Enhbuyant Lhagvajav, Steven Msowoya, Malek Qutteina, Jayanth Kumar
1
Sunita Kishor
1
Sunsari Technical College Journal
1
Superior Health Council
1
Sur, P.J.
1
Surgical Unit-based Safety Program
1
Susa Coffey,et al.
1
Susan Nicolai and Carl Triplehorn
1
Susanne Bartig
1
Susanne Jaspars and Hisham Khogali
1
Sustainability
1
Sustainable Clubfoot Care in Bangladesh
1
Süß, W.
1
Sv Madhu, S. Srivastava
1
Svensson, K.
1
Swain, K.D., Pillay, B.J. & Kliewer, W.
1
Swarts, L.
1
Swaziland Paediatric HIV G uidelines 2010 Ministry of Health and Social Welfare
1
Swe, Thida
1
Swedish International Agricultural Network Initiative SIANI
1
Swiss Peace Foundation
1
System Socio Sanitario Regione Lombardia ATS Milano Città Metropolitana
1
Systems for Improved Access to Pharmaceuticals and Services (SIAPS)
1
Szabo, Christopher, Paul
1
Szefler, S. J.
1
Szenenwechsel
1
Sæbønes, A., Bieler, R. B., Baboo, N., et al
1
T. Bingham
1
T. Bleicker
1
T. Boyles, M. Mendelson
1
T. Chitashvili, S. Holschneider, O. Annie Clark
1
T. D. Vloet
1
T. da Encarnação Sá-Guimarães, E. Seam Lima de Alvarenga et al.
1
T. Driscoll
1
T. Fernández Dávil, P. A. Hidalgo Andrade, F. G. Torres Toala et al.
1
T. Fountaine, J. Lembong, R. Nair, et al.
1
T. Frieden
1
T. Groshkova
1
T. Islam, T. Hiatt, C. Hennig, et al.
1
T. Jaenisch, K.D. Rosenberger, C. Brito, et al
1
T. Jans
1
T. Johnson, Ph.D., et al.
1
T. Jones and J. Bedford
1
T. K. Banerjee
1
T. K. Phillips
1
T. Kasrashvili
1
T. Leenstra, MD, PhD
1
T. Lievens
1
T. M. Achenbach
1
T. Mahon and S. Cavill
1
T. Maier
1
T. Maimakov, L. Sadykova, Z. Kalmataeva, et al.
1
T. Markabaeva
1
T. Mtonga
1
T. Munie
1
T. Mwoma
1
T. N. do Pradoa
1
T. N. Saw
1
T. Nakari
1
T. Ngoato
1
T. Osman
1
T. Powell-Jackson
1
T. Rahman
1
T. Rhodes
1
T. S. Moriyama
1
T. Samudio
1
T. Schaberg, T. Bauer, F. Brinkmann, et al.
1
T. Seutloali
1
T. T.T. Dinh
1
T. Welsh
1
T. Wenzel
1
T. Younga and M. Clarke
1
T. Zurashvili
1
T.N. Do
1
Tabitha Hrynick, T.
1
Tageldin, M.A.
1
Taha, H.
1
Takarinda, Kudakwashe C., Lydia K. Madyira, Mutsa Mhangara, Victor Makaza, Memory Maphosa, Simbarashe Rusakaniko, Peter H. Kilmarx, Tsitsi Mutasa-Apollo, Getrude Ncube, and Anthony D. Harries
1
Tamara Adrián-Hernandez,Elham Atalla, George Ayala et al.
1
Tambo, Ernest
1
Tanabe M. et al.
1
Tanadgoma
1
Tang, Shenglan
1
Tangermann, J.
1
Tania Barham, Randall Kuhn, Jane Menken et al.
1
Tanzania Commission for AIDS (TACAIDS)
1
Tanzania Food & Drugs Authority (TFDA)
1
Tanzania Ministry of Health, Community Development, Gender, Elderly and Children.
1
Tapash Roy et al.
1
Tapash Roy, Lucy Marci, Rashed H. Chowdhury, Kaosar Afsana, Henry Perry
1
TargetHIV
1
Tarkang EE, Gbogbo S, Lutala PM
1
Tarun Gera, Dheeraj Shah, Paul Garner et al.
1
Tasker, A.
1
Taylor & Francis Group
1
Taylor Francis Online
1
Taylorb, R.
1
TB
1
TB Care
1
TB Care II
1
TB CARE1
1
TB HIV
1
TB/CTA
1
TBFacts.org
1
TDR
1
TDR Program
1
Teach, S.J.
1
Technology Transfer and Research Translation Directorate of the Ethiopian Public Health Institute
1
Tefera, S.
1
Teferi, M.
1
Tegally, H.
1
tein, D. J.et al.
1
Teklemariam M., Assefa A., Kassa M., et al.
1
Teklu, Hailemariam, Aluta Sebhatu, and Tesfayi Gebreselassie
1
Tekpa, G., Fikouma, V., Marada, R:M. et. al.
1
Teleducacion Facultad de Medicina Universidad de Antioquia
1
TelessaudeRS, Ministerio da Saude Brasil
1
Telligen, Quality Innovation Network National Coordinating Center, Centers for Medicare & Medicaid Services (CMS)
1
Templin T: et al.
1
Templin, T.
1
Tennisson I.
1
TERRE DES FEMMES
1
Terres des Femmes
1
Terzic, C.P. et al.
1
Tesfaye K.
1
Teshome H.
1
Tessum, C.
1
Thabet, A.M. & Thabet, S.S.
1
Thacher, Emily
1
The African Child Policy Forum (ACPF)
1
The Alliance for Child Protection in Humanitarian Action
1
The Alliance for children protection in humanitarian action
1
The American Journal of Tropical Medicine and Hygiene
1
The Asia Foundation
1
The Association of Physicians of India
1
The Audit Service Sierra Leone
1
The Australian College of Pharmacy
1
The Boston Medical Center
1
The Boston Medical Center/ AVON Foundation for Women
1
The British Medical Journal (BMJ)
1
The Cameroon Academy of Sciences
1
The Center for HIV Law Policy
1
The Centre for Global Mental Health &the Mental Health Innovation Network
1
The Chatham House
1
The Child Protection Initiative, Save the Children
1
The Cochrane HIV
1
The Collaborative Africa Budget Reform Initiative (CABRI)
1
The Collaborative Initiative for Paediatric HIV Education and Research (CIPHER) Global Cohort Collaboration
1
The Dag Hammarskjöld Foundation and ReAct
1
The Department of Social Development
1
The DHS Program ICF
1
The Economic Commission for Africa (ECA)
1
The Economist Intelligence Unit (EIU)
1
The Empowered Fe Fes
1
The EMSA Student Task Force for Digital HealthThe European Medical Student's Association (EMSA)- Association Européenne des Étudiants en Médecine
1
the Essential Drugs Programme, the PHC
1
The Estonian Ministry of Justice
1
The Ethiopian Public Health Institute
1
The European AIDS Clinical Society (EACS)
1
The European Respiratory Journal
1
The Focus Group Consulting
1
The Georg Institute for Global Health India
1
The Global Forum on MSM and HIV (MSMGF)
1
The Global Library of Women’s Medicine by Sapiens Publishing
1
The Global Nutrition Cluster, UNICEF
1
The Global Virology Therapy Monitor Team, Ipsos Healthcare
1
The Government of Malawi
1
the Government of Sierra Leone, the Medical Research Centre, the University of Sierra Leone, the Royal Tropical Institute (KIT), Text to Change, and MannionDaniels
1
The Government of Uganda
1
The Government of Zambia
1
The Governments of Burkina Faso and Norway, the Bill & Melinda Gates Foundation, and the World Bank Group
1
The Health & Education Advice & Resource Team (HEART)
1
The Indonesian Society of Endocrinology Task Force on Thyroid Diseases
1
The International Center for AIDS Programm
1
The International Federation of Medical Students’ Associations (IFMSA)
1
The International Journal of Psychosocial Rehabilitation
1
The International Spinal Cord Association
1
The International Textbook of Leprosy
1
The Irish Hospice Foundation, et al.
1
The Johns Hopkins and the International Federation of Red Cross and Red Crescent Societies
1
The Journal of Allergy and Clinical Immunology
1
The Journal of Child Psychology and Psychiatry
1
The Journal of Global Health
1
The Journal of Headache and Pain
1
The Journal of Infectious Disease
1
The Journal of Maternal-Fetal & Neonatal Medicine
1
The Kings Fund
1
The Kitchener Downtown Community Health Centre, et al.
1
The Lancet Commissions
1
The Lancet Healthy Longevity Volume 2, Issue 6e340-e351June 2021
1
The Lancet Journal
1
The Lancet Regional Health - Americas
1
The Lancet Regional Health – Americas
1
The Lancet Respiratory Medicine Commission
1
the Liberia Institute of Statistics and Geo-Information Services (LISGIS) and the University of Liberia Pacific Institute of Research and Evaluation (UL-Pire)
1
The McGraw-Hill Companies
1
The MEDBOX Team
1
The Ministry of Health
1
The Montpellier Panel
1
The MOST Project
1
The National Child Traumatic Stress Network
1
The National Formulary Committee, National Drug Policy, DOH Philippines
1
The National Institute For Communicable Diseases, South Africa
1
The New England Journal of Medecine
1
The New England Journal of Medicine
1
The New York Times
1
The Open AIDS Journal
1
The Open Infectious Diseases Journal
1
The Open Public Health Journal
1
The Pact
1
The Partnership for Maternal, Newborn & Child Health
1
The Professional Counselor (TPC)
1
The Republic of Tajikistan
1
The Republic of the Union of Myanmar, Ministry of Environmental Conservation and Forestry, National Environmental Conservation Committee
1
The Republic of the Union of Myanmar, Ministry of Health and Sports, Department of Medical Research, Department of Public Health, Department of Medical Services, UNFPA
1
The Republic of the Union of Myanmar, Ministry of Health and Sports, Department of Public Health, Child Health Division
1
The Republic of the Union of Myanmar, Ministry of Health and Sports, Department of Public Health, Department of Medical Services and UNFPA
1
The Republic of the Union of Myanmar, Ministry of Health, Department of Health, National Tuberculosis Programme
1
The Review on Antimicrobial Resistance
1
The ROTA Council
1
The Royal College of Anaesthetists
1
The Royal Society Publishing
1
The Sentinel Project
1
The SMERU Research Institute, UNICEF
1
The South African Cochraine Centre
1
The Standard for Spiritual Care & Education et al
1
The Technical and Operational Performance Support Program
1
The Uganda Gazette
1
The UN Security Council and Climate Change
1
The University of Sydney
1
The Water and Sanitation Program
1
The William J. Clinton Foundation
1
The World Bank
1
Theilmann, M.
1
Theingy Aye et al.
1
TheLancet
1
Thembelihle Hlophe, S.
1
Thoko Ndaba1, Myra Taylor, Musawenkosi Mabaso
1
Thomas Chantereault and Ezzedine Bouzid
1
Thomas Jans Yesim Taneli Andreas Warnke
1
Thomas, L.
1
Thomas, L.S., E. Buch and Y. Pillay
1
Thomas, M. and Ninomiya, A.
1
Thompson, J.L.
1
Thomson, D., Shivanandan, J. & Brown, T.
1
Thomson, D., Shivanandan, J. &
1
Thomson, M.C.
1
Thomson, R.
1
Thornicroft G, Alem A, Antunes Dos Santos R, et al.
1
Thriemer K, Katuala Y, Batoko B, Alworonga J-P, Devlieger H, et al.
1
Thrul, J.
1
Ties Boerma, Colin Mathers, Carla AbouZahr, Somnath Chatterji, Daniel Hogan and Gretchen Stevens
1
Tigray Health Bureau
1
Tigrey Health Bureau
1
Tilahun Tadesse, B., E. A. Ashley, S. Ongarello et al.
1
Tindyebwa, D.
1
Tippy Tap
1
Tirados, I.
1
Tisiligianni, I.
1
Titus, M., Hendricks, R., Ndemueda, J., McQuide, et al
1
Tjaden, N.B.
1
TK Sundari Ravindran
1
Tol, Wietse A. , Song, Suzan, Jordans, Mark J. D.
1
Tom Corsellis and Antonella Vitale
1
Tonelli, M.
1
Torales, G.
1
Toronto Public Health
1
Torres, A.
1
Torres-Rueda S.
1
Toru Hifumi et al.
1
Toumi A.
1
Towards a Safer World
1
Traidl-Hoffmann, C.
1
Training for Health Equity Network (THEnet)
1
Transactions of the Royal Society of Tropical Medicine and Hygiene
1
Transatlantic Taskforce on Antimicrobial Resistance (TATFAR)
1
Trauma & Gewalt
1
Travis Yates, Jelena V. Allen, Myriam Leandre Joseph et al.
1
Treat All
1
Treat Asia (Therapeutics Research, Education, AIDS Training)
1
Treudler, R.
1
Trials
1
Trocaire
1
Tromp, J.
1
Trujillo, C.
1
Tsiligianni, I.
1
Tsollekile, L.P.
1
Tudorache, E. et al.
1
Tufts University
1
Tufts University, Oxfam
1
Tuija Aro and Timo Ahonen
1
Tukahebwa, E. et al
1
TUN, Waimar, et al.
1
Tunesian Federation of sport for persons with disabilities
1
Turale S., Nantsupawat A.
1
Turco, J.V. et al.
1
Turkova, A.
1
Tylor & Francis
1
U. Hausmann
1
U. Ramtekkar
1
U. Williams
1
U.l Ramtekkar
1
u.r.d.
1
U.S Department of health and human service
1
U.S. Agency for International Development Office of Inspector General (USAID)
1
U.S. Department of Homeland Security
1
U.S. Department of Health and Human Services
1
U.S. Department of Health and Human Services, Agency for Toxic Substances and Disease Registry (ATSDR)
1
U.S. Department of Health and Human Services. Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases
1
U.S. Department of Human Services
1
U.S. Department of Veterans Affairs
1
U.S. Food & Drug Administration
1
U.S. Global Malaria Coordinator
1
U.S. Pharmacist
1
U.S. Presidents Malaria Initiative
1
U.S. President’s Malaria Initiative (PMI), CDC, USAID, et al.
1
UBSKM, DJI
1
UCL Institute for Global Health and Development Education Research Centre, Institute of Education
1
Uganda AIDS Commission
1
Uganda Bureau of Statistics & The DHS Program
1
Uganda Ministry of Health
1
Uganda National Action on Physical Disability (UNAPD)
1
Ugurlu, M.
1
uhoza, Dieudonné Ndaruhuye, Pierre Claver Rutayisire, and Aline Umubyeyi.
1
Uisso, C.
1
UK Aid
1
UK Health Security Agency
1
UKAID, APHRC, Population Counc
1
UKE Hamburg
1
Ulman, Y.L.
1
Ulrich Hoffmann, Anita Idel, Tobias Reichert, Hans R. Herren et al.
1
Umbas, R., S. Hardjowijoto, F. Safriadi, et al.,
1
Umited Nations Popuilation Fund UNFPA
1
Umweltbundesamt
1
UN Children´s Fund
1
UN Children´s Fund UNICEF
1
UN Convention to Combat Desertification
1
UN Department of Economic and Social Affairs
1
UN Department of Safety and Security
1
UN DESA
1
UN Development Programme UNDP
1
UN Development Programme, UN High Commissioner for Refugees
1
UN Economic and Social Commission for Asia and the Pacific
1
UN Educational, Scientific and Cultural Organization
1
UN Educational, Scientific and Cultural Organization UNESCO
1
UN High Commissioner for Refugees UNHCR, TANGO
1
UN Office for the Coordination of Humanitarian Affairs (OCHA)
1
UN Office for the Coordination of Humanitarian Affairs OCHA
1
UN Office of the High Commissioner for Human Rights, UN Mission in South Sudan
1
UN Partnership to Promote Rights of People with Disabilites
1
UN Security Council, UN General Assembly
1
UN Sustainable Development Solutions Network (SDSN)
1
UN UN Environment Programme UNEP
1
UN United Nations
1
UN Women UNODC
1
UNA
1
UNAIDS, UNICEF
1
UNCCD
1
UNCEF
1
UNCTAD
1
UNDP – Government of India - SMRC Study
1
UNDP (United Nations Development Programme)
1
UNDP, IRGT, UNFPA, UNAIDS, WHO, USAID, PEPFAR, UCSF Center of Excellence for Transgender Health, Johns Hopkins Bloomberg School of Public Health
1
UNFPA ESARO
1
UNFPA–UNICEF Joint Programme on Female Genital Mutilation
1
UNHCR (The UN Refugee Agency)
1
UNHCR, UNICEF, IRC
1
UNHCR, WHO
1
UNHR
1
Uni Bielefeld
1
Uni Heidelberg
1
UNICEF and UNFPA
1
Unicef Co. UK
1
UNICEF India
1
UNICEF Kosovo in cooperation with Kosovo Health Foundation
1
UNICEF Sudan
1
UNICEF, FiA Foundation
1
UNICEF, Gobierno Bolivariano de Venezuela, et al.
1
Unicef, OPAS
1
UNICEF, WHO, Wellstart International
1
Unicef, World Bank Group
1
UNICEF, World Health Organisation
1
UNICEF, World Health Organisation (WHO)
1
unicef, Український інститут соціальних досліджень імені О. Яременка, Видавництво “К.І.С.”, макет
1
unicef, Український інститут соціальних досліджень імені Олександра Яременка,Дизайн, верстка, друк – ТОВ ВПК «ОБНОВА»
1
UNICF
1
Unidad de Estudios División Política Comercial e Industrial
1
Unidad de vigilancia de la Salud, Gobierno de la répubica de Honduras
1
UNIECF
1
UNIFEC
1
UNION
1
Union for International Cancer Control (UICC)
1
Union Internationale Contra la Tuberculose et les Maladies Respiratoires
1
Unión Internacional Contra la Tuberculosis y Enfermedades Respiratorias
1
Unique Kulima
1
Unite for Children Unite against AIDS
1
UNITE FOR DIABETES PHILIPPINES
1
United Nations - Environment Management Group (EMG)
1
United Nations agencies, the World Bank and the European Commission
1
United Nations and Partners
1
United Nations Children's Fund (UNICEF) & World Health Organisation (WHO)
1
United Nations Children’s Fund (UNICEF), Global Water Partnership (GWP)
1
United Nations Conference on Trade and Development
1
United Nations Department of Economic and Social Affairs (DESA)
1
United Nations Department of Safety and Security (UNDSS)
1
United Nations Development Programme (UNDP) and the Oxford Poverty and Human Development Initiative (OPHI)
1
United Nations Development Programme Bangkok Regional Hub
1
United Nations ECLAC
1
United Nations Economic and Social Commission for Asia and the Pacific (ESCAP)
1
United Nations Educational
1
United Nations Educational, Scientific and Cultural Organization
1
United Nations Educational, Scientific and Cultural Organization (UNESCO)
1
United Nations Educational, Scientific and Cultural Organization Mahatma Gandhi Institute of Education for Peace and Sustainable Development (UNESCO MGIEP)
1
United Nations Enviroment Programme
1
United Nations Environment Programme
1
United Nations High Commissioner for Refugees UNHCR
1
United Nations Human Rights
1
United Nations Institute for Disarmament Research (UNIDIR)ESEARCH
1
United Nations Office for Disaster Risk Reduction UNDRR
1
United Nations Office for the Coordination of Humanitarian Affairs
1
United Nations Office for the Coordination of Humanitarian Affairs (OCHA), Regional Office for Asia and the Pacific (ROAP)
1
United Nations Office on Drugs and Crime (UNODC)
1
United Nations Population Fund
1
United Nations Population Fund (UNFPA)
1
United Nations Population Fund UNPF
1
United Nations publication
1
United Nations Women’s Human Rights and Gender (WRG)
1
United States Agency for International Development (USAID)
1
United States Government Zambia Interagency Team
1
United States Institute of Peace
1
United States Presidents Emergencies Plan for AIDS Relief
1
Unité-Progrès-Justice - Institut national de la statistique et de la démographie - Burkina Faso
1
Univ. Namibia
1
Univ. Zagreb
1
Universidad Complutense de Madrid
1
Universität Duisburg- Essen
1
Universität Heidelberg
1
Universität Tübingen, Abt. f. psychosomatische Medizin und Psychotherapie
1
Université de Montréal
1
Université de Rennes
1
Université Henri Poncare, Nancy, Faculté de médécine de Nancy
1
University of Buffalo
1
University of California, San Francisco
1
University of Cambridge
1
University of Cambridge shelterproject
1
University of Chicago’s Energy Policy Institute
1
University of Malta
1
University of Notre Dame Australia
1
University of Notre Dame, Indiana
1
University of Oxford
1
University of Pittsburgh
1
University of Portland Pilot Scholars
1
University of Pretoria
1
University of Sheffield
1
University of South Florida (USF)
1
University of Washington
1
University of Western Cape
1
University of Wisconsin
1
University of Zurich
1
Universtität Innsbruck
1
UNODC, UNO
1
UNOPS, Stop TB Partnership
1
UNPD
1
UNSCN
1
UNU-WIDER
1
Updated by J.Lees
1
UPenn Collaborative on Community Integratio
1
Uppsala Universitet
1
UPROOT
1
UpToDate
1
Ursula M Read, Edward Adiibokah and Solomon Nyame
1
US Agency for International Development
1
US Agency for International Development USAID
1
US Department of Transportation, Transport Canada
1
US Department of Veterans Afairs
1
US Dept.Health
1
US National Library of Medicine National Institutes of Health (PMC)
1
US President's Malaria Initiative
1
US-China Education Review
1
USAID - From the american People
1
USAID (U.S. President’s Emergency Plan for AIDS Relief)
1
USAID - from the americain people
1
USAID America
1
USAID ASSIST Project
1
USAID From the American People (Health Care Improvement Project)
1
USAID, BASICS
1
USAID, core group, Save the Children, BASICS, MCHIP
1
USAID, Health Finance & Governance
1
USAID, MCHIP
1
USAID, PEPFAR, Health Policy Project
1
USAID, Philippine Statistic Authority
1
USAID, SIAPS (Systems for Improved Access to Pharmaceuticals and Services)
1
USAID, Stop TB Partnership
1
USAID, Strengthening Pharmaceutical Systems SPS
1
USAID, Synergie Project
1
USAID, TBCARE I, TBCARE II
1
USIP
1
UT Health Science Center
1
únete por la niñez
1
Üstün, T.B., Kostanjsek, N., Chatterji, S. & Rehm, J.
1
V&R Unipress
1
V. Andreeva
1
V. Allan
1
V. Cambiano
1
V. Carral
1
V. Delpech
1
V. Fonner
1
V. Fragola
1
V. Galayda
1
V. Habiyambere
1
V. Huber, C. F.Sheng Ng et al.
1
V. Ilyenkova
1
V. J. Wirtz
1
V. Krishnasamy, L.Bulage et al.
1
V. Künzel and L.Schäfer
1
V. M. Kuehlkamp
1
V. Martsynovska
1
V. Msosa, A.L Samateh et al.
1
V. Nankabirwa , J. K. Tumwine, O. Namugga, et al.
1
V. Parikh
1
V. Pathak, Z. Harrington, C. C. Dobler
1
V. Poznyak
1
V. Rashedi
1
V. Rusovich
1
V. Saracenia
1
V. Simms
1
V. Tucci
1
V. Turmine, C. Homm
1
V.Lemmi
1
V.N. Nguyen
1
VA.Saint, and P. Tinnemann
1
Vaartjes, I.C.H.
1
Vaccine
1
Vaduganathan, M.
1
Vaidyanathan, A.
1
Valdoleiros, S. R.
1
Vale, GA et al.
1
Valerie Karr et al.
1
Valérie Arnould
1
Valverde, O.
1
Van Baar, A. et al.
1
van de Pas R., Kolie D., Delamou A., Van Damme W.
1
Van de Voorde, P.
1
van den Dool C., PhD
1
Van Deursen, B.
1
Van Dijck C., Vlieghe E., Cox J.A.
1
van Dyk, L.
1
van Ham C., Reilly K., et al.
1
van Ham, C.
1
Van Katwyk, S. R.
1
Van Ledden, M.
1
Van Ommeren, M.
1
van Ossterhout, J. J.
1
Van PraagO.
1
van Sebille, E.
1
van Straten, B.
1
van Voren, R.
1
van Zandwijk, N.
1
Vanegas, D.
1
Vanham, D.
1
Vanzetti C., Salvo C., Kuschner P. et al.
1
Vanzetti, C.P.
1
Varkey, B.
1
Vassall A.
1
Vassall, A.
1
Vaughan, P.
1
Veeri, B. et al.
1
Veidis, E.M.
1
Velasco-Tirado, V.
1
Velazquez Berumen, A.
1
Veláquez-Ortiz, N.
1
Velho Barreto de Araújo, T.
1
Vengesai A., Naicker T., Kasambala M., et al.
1
VENRO Verband Entwicklungspolitik und Humanitäre Hilfe
1
VENRO-AG Gesundheit
1
Verbeek, J.H.
1
Verein demokratischer Ärztinnen und Ärzte
1
Vereinte Nationen
1
Vergès de López, C.
1
Verhoeven, J.I.
1
Verjeen, M.
1
Verner D.
1
Veronese, Vanessa et al.
1
Verver, S.
1
Verwey and Gopalan
1
Vidya Bhushan Gupta, Priyanka Mehrotra, Naveen Mehrotra
1
Vigaud-Walsh, Francisca
1
Vikram Patel, Dan Chisholm, Tarun Dua et al.
1
Vikram Patel, Melanie Abas, Jeremy Broadhead, et al.
1
Vilajeliu, A, et al.
1
Ville de Goyet, Claude de
1
Villegas ST, Velásquez TL, Hernández SJM
1
Villella, Christina
1
Vincent Gooskens
1
Vincent J.
1
Vineet Bharadwaj, Sandeep Grover, Subho Chakrabarti, et al.
1
Violence and Injury Prevention Unit- Ministry o Health, Kenya
1
Vitillo, B.
1
Vittal Mogasalea, Vijayalaxmi V. Mogasale
1
Vivis
1
Vlad furman, Vera leimane
1
VOICE
1
Voices for Georgia´s Children
1
Vorster, J.M.
1
VSO Ghana
1
Vygen-Bonnet S, Koch J, Bogdan C, et al.
1
W.
1
W. A. Tol
1
W. A. Zule
1
W. Ameyan
1
W. Chirinda
1
W. Haas
1
W.Cheung
1
W.F.Lamb
1
W.K. Townend
1
Waage, J.
1
Wabnitz K., Galle S., Hegge L., et al.
1
Wado, Yohannes Dibaba
1
Wageningen University
1
Wageningen University and Research Centre
1
Wagner, R.C.
1
Wagner, U. et al.
1
Wahedi, K.
1
Wai-him Cheung, Anna Kit-sum Lam & Se-fong Hung
1
Wakefield, M.K.
1
Waldman, L.
1
Walker, A. et al.
1
Walker, J
1
Walker, K.
1
Walker, N.F.
1
Walton D., Arrighi J., et al.
1
Wamai, R.
1
Wambugu, Samuel
1
Wandabwa, M.S.
1
Wander, P.L.
1
Wang, Q.
1
Wang, S., N. Hoohlo, I. Tshabalala, K. Ntoi, and T. Sepetla
1
Wang, W., Do, M., Hembling, J. & Ametepi, P.
1
Wang, Wenjuan, and Rathavuth Hong
1
Wang, Wenjuan, Michelle Winner, Clara Burgert, and Josh Colston
1
Wang, Wenjuan, Soumya Alva, Rebecca Winter, and Clara Burgert
1
Wang, X-R.
1
Wapling, L.
1
War Child International, Women's Refugee Commission
1
War Trauma Foundation
1
Wardlaw, Tessa M.
1
Wardle, H.,
1
Warrell, D.
1
Warsame A.
1
WarTrauma
1
Washington, DC : Futures Group, Health Policy Project
1
Wasserman, S.
1
Water Partnership Program
1
Waterfeld, K.C.
1
Watershed Management Group
1
Watkins, J:W.
1
Watts,N.
1
Watzel B.
1
Wånggren, L.
1
WCC
1
Web of Science
1
Webb, D.
1
Weber, Stephanie
1
WEDC
1
Weerasinghe, I.F., Foneska, P., Dharmaratne, S.D., & Jayatilake, J.A.M.S.
1
Weerawat Manosuthi, Sumet Ongwandee, Sorakij Bhakeecheep et al.
1
Weese, J.
1
Weil, G.J.
1
Weis, J.
1
Weiss, A.
1
Welburn S. C., Beange I. et al
1
Wellcome Open Research
1
Wellcome Trust
1
Welt-Sichten
1
Weltgesundheitsorganisation, Regionalbüro für Europa
1
Wendy Wisbaum, UNICEF España
1
Wenzel, S. E.
1
Werner
1
Werner, D.
1
Werner, D. and B. Bower
1
Wesam B Darawsheh
1
Wesern Cape Government, South Africa
1
Wessells, M., Kostelny, K., and Ondoro, K.
1
Western Cape Government
1
Western Cape Government Health, South Africa
1
Westoff, C.F., F. Ngabo, C. Munyanshongore, M.A. Umubyeyi, and E. Kagame
1
Westoff, Charles F.
1
Westoff, Charles F., and Clara Ladi Ejembi
1
Wexler A.
1
WFP
1
WFP World Food Programme
1
White, Z.
1
Whitmee S., Haines A. et al.
1
Whittemore, Becky J.
1
WHO Regional Office for Europe (WHO
1
WHO and ANESVAD Foundation
1
WHO Collaborating Centre for community participation in palliative care and long term care
1
WHO Country Office for India
1
WHO Framework Convention on Tobacco Control
1
WHO Regional Office for Europe United Nations City
1
WHO SEARO/Department of Control of Neglected Tropical Diseases
1
WHO South Sudan
1
WHO, Columbia University in the city of New York
1
WHO, Department of Reproductive Health and Research, London School of Hygiene and Tropical Medicine, South African Medical Research Council
1
WHO, International Cooperation of Midwifes
1
WHO, TDR
1
WHO, THE END TB STRATEGY
1
WHO, UNFPA, and Escuela Andaluza de Salud Publica Consejeria de Salud
1
WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division
1
WHO, UNODC, MKKH
1
WHO, WEDC, and IWMI
1
WHO,УПН ООН,ЮНЭЙДС
1
WHO=
1
WHOCC AIIMS, UNICEF, UNFPA and USAID
1
Whyms D.
1
Wieland B., Flintan F., et al.
1
Wilder Research
1
Wiley Online Library
1
Wiliams, S.
1
Wilkinson, J.L.
1
Willcox et al
1
Wille, J.
1
Williams, D.
1
Williams, D. et al.
1
Williams, G. et al.
1
Williams, Phoebe CM.
1
Williston, B.
1
Willott C et al.
1
Willy McCourt, W. & Awases, M.
1
Winona State University
1
Winter, Rebecca, Akinlo, Ambrose, and Lia Florey
1
Wirth, James P.
1
Wirtz, Andrea L.
1
Wirtz, V.J.
1
Wisner, B
1
Wisner, B.
1
Wissenschaftlichen Beirats für Familienfragen beim Bundesministerium für Familie, Senioren, Frauen und Jugend
1
Wissenschaftliches Institut der AOK
1
WIZARA YA AFYA MAENDELEO YA JAMII JINSIA, WAZEE NA WATOTO
1
Wiznia, A.
1
Wolrd Health Organization
1
Wolrd Innovation Summir ofr Health WISH
1
Wolters Kluwer
1
Wolters Kluwer Health, Inc.
1
Women for Global Health WGH
1
Women's Refugee Commission, IAWG
1
Women’s Commission for Refugee Women and Children
1
Wonder Goredema Jane Briggs Mupela Ntengu, et al.
1
Wong, M.
1
Woodhead M., F. Blasi, S. Ewig, et al.
1
Woodman, N.
1
Word Health Organization WHO
1
Working Group on Access to Services of the UN Network on Migration, et al.
1
Worku, Abebaw Gebeyehu, Gizachew Assefa Tessema, and Atinkut Alamirrew Zeleke
1
World Bank et al.
1
World Bank Group Staff
1
World Bank Group, and World Health Organization WHO
1
World Bank.
1
World Confederation for Physical Therapy
1
World Council of Churches WCC
1
World Diabetes Foundation
1
World Economic Forum et al.
1
World Federation for Mental Health
1
World Federation of Neurology
1
World Federation of Societies of Anaesthesiologists
1
World Food Programme
1
World Food Programme (WFP)
1
World Government Summit, Sustainable Development Solutions Network
1
World Health Organisation (WHO), Regional Office for Eastern Management
1
World Health Organisation Zimbabwe
1
World Health Organisation, International Labour Organization
1
World Health Organization (Bangladesh)
1
World Health Organization (Cambodia)
1
World Health Organization (Pacific Region)
1
World Health Organization (Regional Office for South-East-Asia)
1
World Health Organization (South-East-Asia)
1
World Health Organization (WHO) - Regional Office for South-East Asia
1
World Health Organization (WHO) and DOH Philippines
1
World Health Organization (WHO) and The World Bank (WB)
1
World Health Organization (WHO) Regional Office for the Eastern Mediterranean
1
World Health Organization (WHO), Alliance for Health Policy and Systems Research
1
World Health Organization (WHO), Department of Mental Health and Substance Abuse
1
World Health Organization (WHO), Food and Agriculture Organization of the United Nations (FAO) and World Organisation for Animal Health (OIE)
1
World Health Organization (WHO), International Pharmaceutical Federation (FIP)
1
World Health Organization (WHO), Strategic and Technical Advisory Group for Neglected Tropical Diseases, Working Group on Monitoring and Evaluation
1
World Health Organization (WHO), The Global Fund, Gavi et al.
1
World Health Organization (WHO), World Bank, Global Financing Facility (GFF) et al.
1
World Health Organization (WHO)
1
World Health Organization - Regional Office for South-East Asia
1
World Health Organization - Regional Office South-East Asia
1
World Health Organization Eastern Mediterranean
1
World Health Organization South-East Asia Region
1
World Health Organization WHO (Africa)
1
World Health Organization WHO and International Atomic Energy Agency IAEA
1
World Health Organization WHO and Internationl Federation of the Red Cross ICRC
1
World Health Organization WHO India
1
World Health Organization WHO Regional Office for South-East Asia
1
World Health Organization WHO Western-Pacific Region
1
World Health Organization WHO, Regional Office for Africa
1
World Health Organization WHO, CDC, UNHCR
1
World Health Organization WHO, Food and Agriculture Organization FAO, World Organization for Animal Health OIE
1
World Health Organization WHO, Food and Agriculture Organization of the United Nations FAO
1
World Health Organization WHO, International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE)
1
World Health Organization WHO, Regional Office Africa
1
World Health Organization WHO, Regional Office for Europe, et al.
1
World Health Organization WHO, SAGE
1
World Health Organization WHO, Stop TB
1
World Health Organization, Stop TB Department
1
World Health Organization, CDC, GTSS et al.
1
World Health Organization, et al.
1
World Health Organization, ICRC, MSF, et al.
1
World Health Organization, Imperial College London
1
World Health Organization, Regional Office South-East Asia
1
World Health Organization, Sout-Easr Asia
1
World Health Organization, South-East Asia
1
World Health Organization, TB HIV working group, Stop TB Partnership
1
World Health Organization, UN Office for the Coordination of Humanitarian Affairs, UN Mission for Ebola Emergency Response
1
World Health Organization, UNICEF, United Nations Population Fund
1
World Health Organization, Western Pacific
1
World Health Organization, World Heart Federation, World Stroke Organization
1
World Health Organization,et al.
1
World Health Organization. Regional Office for South-East Asia
1
World Health Organization/Europe
1
World Health Organizationl
1
World Medical Association
1
World Meteorological Organization WMO
1
World Metrological Organisation - WMO
1
World Organisation for Animal Health
1
World Organisation for Animal Health WOAH
1
World Organisation for Animal Health, World Health Organization (WHO), Food and Agriculture Organization (FAO)
1
World Psychiatric Association
1
World Psychiatry
1
World Vision Sénégal
1
World Vision, International Research Institute for Climate and Society
1
World Wildlife Fund for Nature WWF
1
Wounds International
1
WPSAR
1
Wrench, W.
1
WRH
1
Wright G.D.
1
Wright J.E., Werkman M., Dunn J.C. et al
1
Wright, J.
1
Write State University Dayton
1
Wroe, E.B.
1
WSP - Water and Sanitation Program
1
X. Salazar
1
Xiaoxu Wu, Yongmei Lu, Sen Zhou et al.
1
Xiaoyan Ke, Jing Liu
1
Xu K., Soucat A., Kutzin J., et al.
1
Y .V. Kruglov
1
Y. Arafat, R.Kabir, A.A.Masud
1
Y. Cheng
1
Y. Gilleece
1
Y. Keynan, D. Marin et al.
1
Y. M. F. Moreno
1
Y. M. Saw
1
Y. Santa-Ana-Tellez et al.
1
Y. Sugiura
1
Y. Tabi
1
Y. Tadesse, N. Gebre, S. Daba, et al.
1
Y. Takashima
1
Y. Taneli
1
Y. Tercüman
1
Y. W. Olagbuji
1
Y. Yu
1
Y. Zhang
1
Y.-H. Jin
1
Yale, G.
1
Yan I.
1
Yap, J.
1
Yaria, J.
1
Yassi, A.
1
Yawalker, S.
1
Yeap, C.E., Ibrahim, H., Van Dort, S., et al.
1
Yebyo, Henock G., Mussie A. Gebreselassie, and Alemayehu B. Kahsay
1
Yglesias_González
1
Yimer, G. et al.
1
Yohaness Garoy E., Y. Berhane Gebreab, O. Okoth Achila et al.
1
Yolaine Glèlè-Ahanhanzo, Alphonse Kpozèhouen, Noël Moussiliou Paraïso, Patrick Makoutodé, Chabi O. Alphonse Biaou, Eric Remacle, Edgard-Marius Ouendo, Alain Levêque
1
Yon, D.K. et al.
1
Yoo, J.E.
1
Yotsu,R.R.
1
Yourkavitch, Jennifer
1
Yu C, Lougee D, Murno JR
1
Yu, J. et al.
1
Yuen K. Y.
1
Yuniadi, Y., A.E. Tondas, D.A. Hanafy, et al.,
1
Yusuf, S.
1
Yuyun, M.F.
1
Z. Brihnu
1
Z. Chirwa
1
Z. Diaz-Bello, C. Colmenares, et al.
1
Z. Qiao
1
Z. Suarez
1
Z. T. Gavry
1
Z. Z. Aunga
1
Z.-S. Cheng
1
Zafar, S.
1
Zaidel, E.J.
1
Zaidi, Shehla
1
Zaman, M.
1
Zamani's Lab, R. et al.
1
Zanzibar AIDS Commission (ZAC)
1
Zar, H.J.
1
Zayeri, F.
1
Zerbini E. De Sandro j., et al.
1
Zerbo P., J. Millogo-Rasolodimby, O. G.Nacoulma-Ouedraogo
1
Zhang, H-X.
1
Zhang, J.
1
Zhang, X.
1
Zhao,Q.
1
Zhu, Anna
1
Ziaggi, G.
1
Zida, A.
1
Zifodaya, J.
1
Zimbabwe National Statistics Agency (ZIMSTAT)
1
Zimmer, C, J. Corum and S. Wee
1
Zinsou, C.
1
Zipper, S.
1
Zoila Caridad Moros, Ferdinando Liprandi, Flor Helene Pujol
1
Zulema Torres G., Victoria Pickett S. et al
1
Zulfiqar A. Bhutta, Zohra S. Lassi, George Pariyo and Luis Huicho
1
Zulianlly Rojas, Saylee Ochoa, Román Millán, et al.
1
Zuurmond, M., L.M. Banks, P. Aryal, et al.
1
Zürcher Hochschule für Angewandte Wissenschaften (zhaw)
1
А. А. Шульдяков, Ю. Б. Барыльник, Е. П. Ляпина et al.
1
А.В.Владзимирский, Т.В.Риден, Н.В.Ледихова et al.
1
Айме Меос, Ану Суси, Эвели Месикяпп et al.
1
Александрович Ю.С., Алексеева Е.И., Бакрадзе М.Д., et al.
1
Анджела Ми, Тибо ле Пишон, Коэн Буссинк e tal.
1
Андрей Клепиков, Людмила Шурпач, Виктор Исаков et al.
1
АНО «Наш Солнечный мир», Международная ассоциация Autism-Europe
1
Антонова А. А., Бачило Е. В., Барыльник Ю. Б.
1
Артымук Н. В., Баев О. Р., Белокриницкая Т. Е. et al.
1
Байярд Робертс, Ніно Махашвілі, Джана Джавахішвілі et al.
1
Барцалкина В.В. et al.
1
Бачило Е. В., Барыльник Ю. Б.
1
Бачило Е. В., Барыльник Ю. Б., Антонова А. А.
1
Беверли Коллин, Филипп дю Крос, Натан Форд, Джо Хатчинсон, Наташа Льюэр, Лесли Шэнкс, Франсис Варэн
1
В.В. Юдина, Н.С. Макаров, Г.К. Юдина et al.
1
В.Ф. Беженарь, Э.К. Айламазян, И.Е. Зазерская et al.
1
Васильева Ирина Анатольевна, Самойлова Анастасия Геннадьевна, Эргешов Атаджан Эргешович et al.
1
Васильева Лидия Львовна
1
ВОЗ и Международная организация по проблемам болезни Альцгеймера
1
Всеми́рная организа́ция здравоохране́ния
1
Всемирная организация здравоохранени (UNHCR)
1
Всемирная организация здравоохранения (World Health Organization Europe)
1
Всемирная организация здравоохранения (World Health Organization)
1
Всемирная организация здравоохранения (Европа)
1
Всемирная организация здравоохранения (Европейское)
1
Всемирная организация здравоохранения. Европейское региональное бюро
1
Г-жа M. Mansfeld
1
Г-н Z. T. Gavry
1
Г. Е. Иванова, И. Н. Баландина, Т. Т. Батышева et al.
1
Гаврилова С.И, Aлесенко А.В., Mолочкина Е.М. et al.
1
ГБОУ ВПО «Нижегородская государственная медицинская академия»
1
Глобальный фонд
1
Д-р M. Dara
1
Д-р Огтай Гозалов
1
Д. А. Энарсон, Г. Л. Ридер, Т. Арнадоттир et al.
1
Дёмин Андрей Константинович, Коротаев Андрей Витальевич, Халтурина Дарья Андреевн
1
Департамент "Остановить туберкулез", ВОЗ
1
Департамент по ВИЧ/СПИД, Департамент «Остановить ТБ», Всемирная организация здравоохранения
1
Детский фонд Клиника Тартуского университета, Клиника Тартуского университета et al.
1
Детский фонд ООН (ЮНИСЕФ)
1
Детский фонд ООН UNICEF, Всеукраинский союз молодежных общественных организаций,«Христианская ассоциация молодых людей Украины» (YMCA Украины
1
Дженнифер Батлер
1
Джорджа Айалы
1
Е.А. Катунина, Ю.Н. Бездольный
1
Е.Л. Никонов, С.В. Кашин,Р.О. Куваев, et al.
1
Ж.В. Альбицкая
1
Жан-Люк Лемахье, Ангела Ме, Хлое Карпентье et al.
1
Жилберт Жерро, Николас Кларк
1
И. Ерамова, В. Ильенкова,
1
И.И. Марценковская, Ю.А. Войтенко, К.В. Дубовик et. al.
1
Камкин Евгений Геннадьевич, Костенко Наталья Алексеевна et. al.
1
Карелина Д.Д., Кром И.Л., Барыльник Ю.Б.
1
Київський міжнародний інститут соціології, Державна соціальна служба для сім’ї, дітей та молоді, unicef
1
Колыхалов И.В., Гаврилова С.И.
1
Кэтлин Инглэнд
1
Лукина Е. В., Чернышева О. А., Елисеева В. А.
1
Лукина Е.В. ,Кузнецова Д.Е.
1
Ліса Г. Джейкокс, Одра К. Ленґлі, Крістін Л. Дін
1
Маслюк О. А., Смоленцева И. Г., Амосова Н. А.
1
Медична газета «Здоров’я України»
1
Международный Альянс по ВИЧ/СПИД, AIDS Foundation East West, TRAINING CENTER
1
Международный союз по борьбе с туберкулезом и болезнями легких
1
Международный Союз по борьбе с туберкулезом и заболеваниями легких
1
Мосолов С.Н., Костюкова Е.Г., Цукарзи Э.Э.
1
МФ «Відродження»
1
Назим Агазаде, Ирина Михайловна Никольская, Игорь Валерьевич Добряков et al.
1
Научно-практический клинический центр диагностики и телемедицинских технологий Департамента здравоохранения города Москвы
1
нтон Харрис, Дермот Махер, Стивен Грэхем et al.
1
О. Л. Корольчук
1
О. М. Балакірєва,Т. В. Бондар, Ю. Ю. Приймак et al.
1
О.А. Жукова, Ю.Б. Барыльник, И.Л. Кром
1
О.М. Балакірєва,Т.В. Бондар, Н.О. Рингач et al.
1
О.М. Балакірєва,Т.В. Бондар, Я.О. Сазонова et al.
1
Общественная палата Российской Федерации
1
Оганна Киракосян
1
Оксана Залесская
1
Организация Объединенных Наций
1
Организация Объединенных Наций, UNODC
1
пер. с англ. М. Шихиревой, Международная ассоциация Autism-Europe
1
Пінчук І.Я., Бабова К.Д., Го-женка А.І.
1
Раздорская В. В., Воскресенская О. Н., Юдина Г. К.
1
Региональная благотворительная общественная организация
1
Российский государственный медицинский университет им. Н.И. Пирогова Кафедра неврологии и нейрохирургии лечебного факультета д.м.н., доцент Е.А. Катунина, к.м.н. Ю.Н. Бездольный
1
С. Г. Сукиасян
1
С. Н. Авдеев , Е. В. Волчкова , О. М. Драпкина, et al.
1
Самойлова Д. Д., Барыльник Ю. Б.
1
Сергей Богданов, Оксана Залесская
1
Сиволап Ю.П.
1
Сильвия Бразилиану, Патрисия Хохграф , Абдула Диуф et al.
1
Сорос-Кыргызстан
1
Союз охраны психического здоровья, Issa, world council for psychotheraphy et al.
1
Т. В. Короткевич, В. П. Максимчук, Е. В. Воронцова, А. А. Кралько, И. А. Белаец, О. И. Глаголева
1
Т.А. Солохина, проф. В.С. Ястребов, Л.С. Шевченко et al.
1
Український інститутсоціальних дослідженьімені Олександра Яременка, unicef, emcdda
1
УПРАВЛЕНИЕ ОРГАНИЗАЦИИ ОБЪЕДИНЕННЫХ НАЦИЙ ПО НАРКОТИКАМ И ПРЕСТУПНОСТИ (Вена)
1
УПРАВЛЕНИЕ ОРГАНИЗАЦИИ ОБЪЕДИНЕННЫХ НАЦИЙ ПО НАРКОТИКАМ И ПРЕСТУПНОСТИ Вена
1
ФГБНУ «Научный центр психического здоровья»
1
ФГБУ «НАУЧНЫЙ ЦЕНТР ПСИХИЧЕСКОГО ЗДОРОВЬЯ» РАМН
1
Федеральное государственное бюджетное учреждение «Научный центр психического здоровья» Российской академии медицинских наук
1
федеральное государственное бюджетное учреждение центральный научно-исследовательский институт туберкулеза российской академии медицинских наук, Американский международный союз здравоохранения
1
Фонд Организации Объединенных Наций в области народонаселения
1
Центр здоровья и прав человека имени Франсуа-Ксавье Баню и Фонд открытого общества
1
Центр психического здоровья «Стресс»
1
Центр социально-психологической и информационной поддержки «Семья и психическое здоровье»
1
Шабунин А. В., Пушкарь Д. Ю., Касян Г. Р., et al.
1
Щаницын И. Н., Раздорская В. В., Колоколов О. et al.
1
Эко-Вектор
1
Євгеній Польщиков, Олександр Красновський, Оксана Панасенко
1
Інститут психічного здоров’я українського католицького університету видавнича серія «психологія. психіатрія. психотерапія» видання здійснене у партнерстві з українським інститутомкогнітивно-поведінкової терапіїта фондом «Швейцарське бюро співробітництва в Україні»
1
世界卫生组织
1
Interagency Coordination Group on Antimicrobial Resistance IAGG
1
Publication Years
2220-2026
1
2020-2026
2397
2010-2019
4947
2000-2009
681
1990-1999
55
1980-1989
4
1970-1979
1
1960-1969
2
-2010--2001
1
Category
Countries
2680
Clinical Guidelines
660
Public Health
444
Women & Child Health
386
Key Resources
233
Capacity Building
125
Pharmacy & Technologies
79
General Guidelines
8
Protection & Security
1
Toolboxes
COVID-19
961
Mental Health
816
HIV
608
TB
516
Planetary Health
352
Disability
268
Caregiver
246
NCDs
221
NTDs
220
Refugee
212
AMR
202
Rapid Response
190
Ebola
185
Global Health Education
124
Conflict
117
Pharmacy
112
Health Financing Toolbox
107
Zika
86
Natural Hazards
74
Social Ethics
56
Cholera
40
Polio
37
Specific Hazards
33
Typhoon
2
Health Financing
2
South Sudan
1
Cardiovascular disease (CVD) is the leading cause of global deaths, with the majority occurring in low- and middle-income countries (LMIC). The primary and secondary prevention of CVD is suboptimal throughout the world, but the evidence-practice gaps are much more pronounced in LMIC. Barriers at the
...
patient, health-care provider, and health system level prevent the implementation of optimal primary and secondary prevention. Identification of the particular barriers that exist in resource-constrained settings is necessary to inform effective strategies to reduce the identified evidence-practice gaps. Furthermore, targeting modifiable factors that contribute most significantly to the global burden of CVD, including tobacco use, hypertension, and secondary prevention for CVD will lead to the biggest gains in mortality reduction. We review a select number of novel, resource-efficient strategies to reduce premature mortality from CVD, including: (1) effective measures for tobacco control; (2) implementation of simplified screening and management algorithms for those with or at risk of CVD, (3) increasing the availability and affordability of simplified and cost-effective treatment regimens including combination CVD preventive drug therapy, and (4) simplified delivery of health care through task-sharing (non-physician health workers) and optimizing self-management (treatment supporters). Developing and deploying systems of care that address barriers related to the above, will lead to substantial reductions in CVD and related mortality.
more
The World Heart Federation (WHF) has been advocating globally for stronger
legislation and policy regarding cardiovascular disease (CVD) for many years. Now, as focus shifts from global to national progress, we call on members and colleagues to advocate for greater action on CVD in your local setti
...
ngs. This ‘Road to 2018 Toolkit’ provides World Heart Federation members with information
and specific, practical tools to support national CVD advocacy, especially around the United Nations High-Level Meeting on NCDs in 2018.
more
Heart failure with a reduced ejection fraction (HFrEF) is a condition frequently encountered by healthcare professionals and, in order to achieve the best outcomes for patients, needs to be managed optimally. This guideline document is based on the European Society of Cardiology Guidelines for the t
...
reatment of acute and chronic heart failure published in 2016, and summarises what is considered the best current management of patients with the condition. It provides information on the definition, diagnosis and epidemiology of HFrEF in the African context. The best evidence-based treatments for HFrEF are discussed, including established therapies (beta-blockers, ACE-i/ARBs, mineralocorticoid receptor antagonists (MRAs), diuretics) that form the cornerstone of heart failure management as well as therapies that have only recently entered clinical use (angiotensin receptor-neprilysin inhibitor (ARNI), sodium/glucose cotransporter-2 (SGLT2) inhibitors). Guidance is offered in terms of more invasive therapies (revascularisation, implantable cardioverter defibrillators (ICDs) and cardiac resynchronisation therapy (CRT) by implantation of a biventricular pacemaker with (CRT-D) or without (CRT-P) an ICD, left ventricular assist device (LVAD) use and heart transplantation) in order to ensure efficient use of these expensive treatment modalities in a resourcelimited environment. Furthermore, additional therapies (digoxin, hydralazine and nitrates, ivabradine, iron supplementation) are discussed and advice is provided on general preventive strategies (vaccinations). Sections to discuss conditions that are particularly prevalent in sub-Saharan Africa (HIV-associated cardiomyopathy (CMO), peripartum CMO, rheumatic heart disease, atrial fibrillation) have been added to further improve clinical care for these commonly encountered disease processes.
more
Since 2002, development assistance for health has substantially increased,
especially investments for HIV, tuberculosis (TB) and malaria control. We
undertook a systematic review to assess and synthesize the existing evidence in
the scientific literature on the health impacts of these investments
...
more

Development assistance for health (DAH) has increased substantially in recent years and is seen as important to the improvement of health and health systems in developing countries. As a result, there has been increasing interest in tracking and understanding these resource flows from the global hea
...
lth community. A number of datasets, each with its own strengths and weaknesses, are available to track DAH. In this article we review the available datasets on DAH and summarize the strengths and weaknesses of each of these datasets to help researchers make the best choice of which to use to inform their analysis. Finally, we also provide recommendations about how each of these datasets could be improve
more
Erstellen einer Formel mit dem Ergebnis eine konkrete Summe für Deutschland und andere Geberstaaten in Bezug auf eine faire Beitragshöhe an den GFATM zu ermitteln

This report provides an analysis of donor government funding to address the HIV response in low- and
middle-income countries in 2022, the latest year available, as well as trends over time. It includes both
bilateral funding from donors and their contributions to the Global Fund to Fight AIDS, Tub
...
erculosis and
Malaria (Global Fund), UNITAID, and UNAIDS. Overall, the analysis shows that while donor government
funding for HIV increased between 2021 and 2022, this was primarily due to the timing of payments from
the U.S. government and not actual increases in commitments.
more
ABSTRACT
More than 500 million people worldwide live with cardiovascular disease (CVD). Health systems today face fundamental challenges in delivering optimal care due to ageing populations, healthcare workforce constraints, financing, availability and affordability of CVD medicine, and service del
...
ivery.
Digital health technologies can help address these challenges. They may be a tool
to reach Sustainable Development Goal 3.4 and reduce premature mortality from
non-communicable diseases (NCDs) by a third by 2030. Yet, a range of fundamental barriers prevents implementation and access to such technologies. Health system governance, health provider, patient and technological factors can prevent or distort their implementation.
World Heart Federation (WHF) roadmaps aim to identify essential roadblocks on the pathway to effective prevention, detection, and treatment of CVD. Further, they aim to provide actionable solutions and implementation frameworks for local adaptation. This WHF Roadmap for digital health in cardiology identifies barriers to implementing digital health technologies for CVD and provides recommendations for overcoming them.
more
In 2012, all Member States of the World Health Organization (WHO) endorsed a historical target to reduce premature mortality from noncommunicable diseases
(NCD). This commitment was echoed in 2015 by the United Nations Sustainable Development Goals, which included a target to reduce premature morta
...
lity (the
measure of unfulfilled life expectancy and deaths between the ages of 30 and 70 years) from NCD by 30% by the year 2030. The Sustainable Development Goals are especially relevant to cardiovascular disease (CVD), the leading cause of death globally, with increasing prevalence in low- and middle-income countries (LMIC).
more
Background
Access to medicines is important for long‐term care of cardiovascular diseases and hypertension. This study provides a cross‐country assessment of availability, prices, and affordability of cardiovascular disease and hypertension medicines to identify areas for improvement in access
...
to medication treatment.
Methods and Results
We used the World Health Organization online repository of national essential medicines lists (EMLs) for 53 countries to transcribe the information on the inclusion of 12 cardiovascular disease/hypertension medications within each country's essential medicines list. Data on availability, price, and affordability were obtained from 84 surveys in 59 countries that used the World Health Organization's Health Action International survey methodology. We summarized and compared the indicators across lowest‐price generic and originator brand medicines in the public and private sectors and by country income groups. The average availability of the select medications was 54% in low‐ and lower‐middle‐income countries and 60% in high‐ and upper‐middle‐income countries, and was higher for generic (61%) than brand medicines (41%). The average patient median price ratio was 80.3 for brand and 16.7 for generic medicines and was higher for patients in low‐ and lower‐middle‐income countries compared with high‐ and upper‐middle‐income countries across all medicine categories. The costs of 1 month's antihypertensive medications were, on average, 6.0 days’ wage for brand medicine and 1.8 days’ wage for generics. Affordability was lower in low‐ and lower‐middle‐income countries than high‐ and upper‐middle‐income countries for both brand and generic medications.
Conclusions
The availability and accessibility of pharmaceuticals is an ongoing challenge for health systems. Low availability and high costs are major barriers to the use of and adherence to essential cardiovascular disease and antihypertensive medications worldwide, particularly in low‐ and lower‐middle‐income countries.
more
Cardiovascular diseases (CVD) represent the highest burden of disease globally. Medicines are a critical intervention used to prevent and treat CVD. This review describes access to medication for CVD from a health system perspective and strategies that have been used to promote access, including pro
...
viding medicines at lower cost, improving medication supply, ensuring medicine quality, promoting appropriate use, and managing intellectual property issues. Using key evidence in published and gray literature and systematic reviews, we summarize advances in access to cardiovascular medicines using the 5 health system dimensions of access: availability, affordability, accessibility, acceptability, and quality of medicines. There are multiple barriers to access of CVD medicines, particularly in low- and middle-income countries. Low availability of CVD medicines has been reported in public and private healthcare facilities. When patients lack insurance and pay out of pocket to purchase medicines, medicines can be unaffordable. Accessibility and acceptability are low for medicines used in secondary prevention; increasing use is positively related to country income. Fixed-dose combinations have shown a positive effect on adherence and intermediate outcome measures such as blood pressure and cholesterol. We have a new opportunity to improve access to CVD medicines by using strategies such as efficient procurement of low-cost, quality-assured generic medicines, development of fixed-dose combination medicines, and promotion of adherence through insurance schemes that waive copayment for long-term medications. Monitoring progress at all levels, institutional, regional, national, and international, is vital to identifying gaps in access and implementing adequate policies.
more
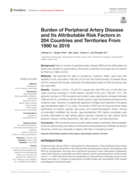
Background: Data on burden of peripheral artery disease (PAD) and its attributable risk factors are valuable for policymaking. We aimed to estimate the burden and risk factors for PAD from 1990 to 2019.
Methods: We extracted the data on prevalence, incidence, death, years lived with disability (YLD
...
s), and years of life lost (YLLs) from the Global Burden of Disease Study 2019 to measure PAD burden. Moreover, the attributable burden to PAD risk factors was also estimated.
Results: Globally, in 2019, 113,443,017 people lived with PAD and 10,504,092 new cases occurred, resulting in 74,063 deaths, 500,893 YLDs, and 1,035,487 YLLs. The absolute numbers of PAD prevalent and incident cases significantly increased between 1990 and 2019, contrasting with the decline trends in age-standardized prevalence and incidence rates. However, no statistically significant changes were detected in the global age-standardized death or YLL rates. The burden of PAD and its temporal trends varied significantly by location, gender, age group, and social-demographic status. Among all potentially modifiable risk factors, age-standardized PAD deaths worldwide were primarily attributable to high fasting plasma glucose, followed by high systolic blood pressure, tobacco, kidney dysfunction, diet high in sodium, and lead exposure.
Conclusion: PAD remained a serious public health problem worldwide. More strategies aimed at implementing cost-effective interventions and addressing modifiable risk factors should be carried out, especially in regions with high or increasing burden.
more
The Global Burden of Disease Study (GBD) began 30 years ago with the goal of providing timely, valid and relevant assessments of critical health outcomes. Over this period, the GBD has become progressively more granular. The latest iteration provides assessments of thousands of outcomes for diseases
...
, injuries and risk factors in more than 200 countries and territories and at the subnational level in more than 20 countries. The GBD is now produced by an active collaboration of over 8,000 scientists and analysts from more than 150 countries. With each GBD iteration, the data, data processing and methods used for data synthesis have evolved, with the goal of enhancing transparency and comparability of measurements and communicating various sources of uncertainty. The GBD has many limitations, but it remains a dynamic, iterative and rigorous attempt to provide meaningful health measurement to a wide range of stakeholders.
more

Objective: To identify gaps in national stroke guidelines that could be bridged to enhance the quality of stroke care services in low- and
middle-income countries.
Methods: We systematically searched medical databases and websites of medical societies and contacted international organizations.
Co
...
untry-specific guidelines on care and control of stroke in any language published from 2010 to 2020 were eligible for inclusion. We reviewed
each included guideline for coverage of four key components of stroke services (surveillance, prevention, acute care and rehabilitation).
We also assessed compliance with the eight Institute of Medicine standards for clinical practice guidelines, the ease of implementation of
guidelines and plans for dissemination to target audiences.
Findings: We reviewed 108 eligible guidelines from 47 countries, including four low-income, 24 middle-income and 19 high-income countries.
Globally, fewer of the guidelines covered primary stroke prevention compared with other components of care, with none recommending
surveillance. Guidelines on stroke in low- and middle-income countries fell short of the required standards for guideline development;
breadth of target audience; coverage of the four components of stroke services; and adaptation to socioeconomic context. Fewer low- and
middle-income country guidelines demonstrated transparency than those from high-income countries. Less than a quarter of guidelines
encompassed detailed implementation plans and socioeconomic considerations.
Conclusion: Guidelines on stroke in low- and middle-income countries need to be developed in conjunction with a wider category of
health-care providers and stakeholders, with a full spectrum of translatable, context-appropriate interventions.
more
Type 1 diabetes is reported to have significant mortality in Africa. However, there is a paucity of data on pooled estimates of its incidence and prevalence in Africa. This first systematic review and meta-analysis will be conducted to determine the incidence and prevalence of this condition in Afri
...
ca.
more
The epidemiology of adult-onset type 1 diabetes (T1D) incidence is not well-characterized due to the historic focus on T1D as a childhood-onset disease.
This two-site randomised trial compared the effectiveness of a voluntary sector-led, community-based diabetes prevention programme to a waiting-list control group at 6 months, and included an observational follow-up of the intervention arm to 12 months.
Air pollution is one of the leading causes of health complications and mortality worldwide, especially affecting lower-income groups, who tend to be more exposed and vulnerable. This study documents the relationship between ambient air pollution exposure and poverty in 211 countries and territories.
...
Using the World Health Organization’s (WHO) 2021 revised fine particulate matter (PM2.5) thresholds, we show that globally, 7.3 billion people are directly exposed to unsafe average annual PM2.5 concentrations, 80 percent of whom live in low- and middle-income countries. Moreover, 716 million of the world’s lowest income people (living on less than $1.90 per day) live in areas with unsafe levels of air pollution, especially in Sub-Saharan Africa. Air pollution levels are particularly high in lower-middle-income countries, where economies tend to rely more heavily on polluting industries and technologies. These findings are based on high-resolution air pollution and population maps with global coverage, as well as subnational poverty estimates based on harmonized household surveys.
more
Long-term exposure of humans to air pollution enhances the risk of cardiovascular and respiratory diseases. A novel Global Exposure Mortality Model (GEMM) has been derived from many cohort studies, providing much-improved coverage of the exposure to fine particulate matter (PM2.5). We applied the GE
...
MM to assess excess mortality attributable to ambient air pollution on a global scale and compare to other risk factors.
Methods and results
We used a data-informed atmospheric model to calculate worldwide exposure to PM2.5 and ozone pollution, which was combined with the GEMM to estimate disease-specific excess mortality and loss of life expectancy (LLE) in 2015. Using this model, we investigated the effects of different pollution sources, distinguishing between natural (wildfires, aeolian dust) and anthropogenic emissions, including fossil fuel use. Global excess mortality from all ambient air pollution is estimated at 8.8 (7.11–10.41) million/year, with an LLE of 2.9 (2.3–3.5) years, being a factor of two higher than earlier estimates, and exceeding that of tobacco smoking. The global mean mortality rate of about 120 per 100 000 people/year is much exceeded in East Asia (196 per 100 000/year) and Europe (133 per 100 000/year). Without fossil fuel emissions, the global mean life expectancy would increase by 1.1 (0.9–1.2) years and 1.7 (1.4–2.0) years by removing all potentially controllable anthropogenic emissions. Because aeolian dust and wildfire emission control is impracticable, significant LLE is unavoidable.
Conclusion
Ambient air pollution is one of the main global health risks, causing significant excess mortality and LLE, especially through cardiovascular diseases. It causes an LLE that rivals that of tobacco smoking. The global mean LLE from air pollution strongly exceeds that by violence (all forms together), i.e. by an order of magnitude (LLE being 2.9 and 0.3 years, respectively).
more
The article "Capacity-Building in Community-Based Drug Treatment Services" by Michael J. Cole focuses on the global challenges in providing adequate community-based drug treatment services. It highlights the gaps in availability, quality, and access
...
ibility of evidence-based care. The article discusses the principles and strategies for capacity-building at three levels: individual, organizational, and service sector. It emphasizes using an empowerment model, engaging community stakeholders, and creating sustainable practices. The paper also addresses the need for systematic planning, assessment, and collaboration to strengthen drug treatment systems globally.
more