Filter
3833
Text search:
patient
safety
Featured
476
988
Language
3621
130
78
74
46
30
22
20
9
9
9
8
6
4
3
3
3
3
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Document type
2018
696
478
263
142
89
64
23
18
13
12
9
8
Countries
180
127
112
109
109
105
82
82
80
61
59
54
50
49
47
45
44
43
42
38
38
37
37
33
28
26
24
24
23
23
22
21
21
20
19
18
18
18
17
17
15
15
14
12
12
12
11
10
10
10
10
9
9
8
7
6
6
6
6
6
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
663
235
130
113
94
85
44
44
38
36
34
33
28
24
21
20
18
18
18
17
17
17
16
16
16
16
15
14
14
14
14
14
13
13
13
13
13
12
12
11
11
11
11
11
11
10
10
10
10
10
10
10
9
9
8
8
8
8
8
8
8
7
7
7
7
7
7
7
7
7
7
7
7
7
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
6
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
5
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
3
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Publication Years
1124
2328
357
22
2
Category
1349
436
215
185
171
82
72
2
1
Toolboxes
443
267
224
215
213
206
184
154
139
81
77
73
61
61
50
41
30
26
24
23
18
10
10
1
The evolving epidemic of type 2 diabetes mellitus has challenged health-care professionals. It stands among the leading causes of mortality in the present world. It warrants new and versatile approaches to improve mortality and the associated huge quality-adjusted life years lost to it once diagnose
...
d. A possible venue to lower the incidence is to assess the safety and efficacy of various diabetes prevention strategies. Diet and exercise have a well-developed role in the prevention of weight gain and, ultimately, diabetes mellitus type II in high-risk individuals. However, high-risk individuals can also benefit from adjunct pharmacotherapy. In light of this information, we decided to conduct a systematic review of randomized controlled trials. This article summarizes the evidence in the literature on the pharmacological prevention of diabetes in high-risk individuals.
more
Type 2 diabetes in adults
National Institute for Communicable Disease (NICE)
National Institute for Communicable Disease (NICE)
(2023)
CC2
The document provides the NICE Quality Standard for managing Type 2 diabetes in adults (QS209). It outlines evidence-based recommendations for preventing Type 2 diabetes, structured education, continuous glucose monitoring (CGM), medication such as SGLT2 inhibitors, and regular care processes to mon
...
itor complications. The guidelines emphasize individualized care, addressing health inequalities, and improving patient outcomes. They are intended to support healthcare professionals and services in delivering high-quality, equitable diabetes care.
more
Type 1 diabetes in adults
National Institute for Communicable Disease (NICE)
National Institute for Communicable Disease (NICE)
(2023)
CC2
The document provides quality standards for managing Type 1 diabetes in adults, emphasizing areas like structured education, continuous glucose monitoring (CGM), cardiovascular risk management, and diabetic foot assessment. It aims to improve care processes, reduce complications, and enhance
...
patient outcomes through evidence-based and patient-centered approaches. The guidelines also focus on supporting inpatient self-management and ensuring equality and accessibility in diabetes care.
more
The document "Management of Type 2 Diabetes Mellitus" provides comprehensive guidelines for the diagnosis, prevention, and treatment of type 2 diabetes in adults. It emphasizes the importance of individualized glycemic targets, lifestyle interventions like diet and exercise, and the use of medicatio
...
ns such as metformin, SGLT2 inhibitors, and GLP1 receptor agonists to manage blood sugar levels and reduce long-term complications. The document also discusses the screening and management of comorbidities such as hypertension, hyperlipidemia, and diabetic complications like retinopathy, neuropathy, and nephropathy. It highlights the role of diabetes self-management education and support in improving adherence to treatment and patient outcomes. The guidelines are evidence-based and aim to reduce morbidity and mortality associated with type 2 diabetes.
more
The "Primary Healthcare Standard Treatment Guidelines and Essential Medicines List" by the South African National Department of Health provides evidence-based guidelines for diagnosing and managing common medical conditions at the primary healthcare level. This document includes treatment protocols
...
for various health issues, such as infections, chronic diseases, maternal and child health, mental health, and emergency care. It aims to standardize care, promote rational medicine use, and ensure equitable access to essential medications across South Africa. The guidelines emphasize prevention, accurate diagnosis, and efficient treatment strategies to improve patient outcomes.
more
Appropriate use and withdrawal of inhaled corticosteroids (ICS) in patients with chronic obstructive pulmonary disease (COPD)
Román-Rodríguez, M.; Tsiligianni, I.; Wiliams, S.; et al.
International Primary Care - Respiratory Group
(2020)
CC2
The document "Appropriate use and withdrawal of inhaled corticosteroids (ICS) in patients with chronic obstructive pulmonary disease (COPD)" from the IPCRG provides guidance on when to start, adjust, or discontinue ICS in COPD treatment. It highlights the benefits and risks, emphasizing personalized
...
treatment based on patient history, exacerbation frequency, and eosinophil count, while detailing how to optimize bronchodilator use to manage symptoms effectively.
more
The pharmacological management of asthma has changed considerably in recent decades, as it has come to be understood that it is a complex, heterogeneous disease with different phenotypes and endotypes. It is now clear that the goal of asthma treatment should be to achieve and maintain control of the
...
disease, as well as to minimize the risks (of exacerbations, disease instability, accelerated loss of lung function, and adverse treatment effects). That requires an approach that is personalized in terms of the pharmacological treatment, patient education, written action plan, training in correct inhaler use, and review of the inhaler technique at each office visit. A panel of 22 pulmonologists was invited to perform a critical review of recent evidence of pharmacological treatment of asthma and to prepare this set of recommendations, a treatment guide tailored to use in Brazil. The topics or questions related to the most significant changes in concepts, and consequently in the management of asthma in clinical practice, were chosen by a panel of experts. To formulate these recommendations, we asked each expert to perform a critical review of a topic or to respond to a question, on the basis of evidence in the literature. In a second phase, three experts discussed and structured all texts submitted by the others. That was followed by a third phase, in which all of the experts reviewed and discussed each recommendation. These recommendations, which are intended for physicians involved in the treatment of asthma, apply to asthma patients of all ages.
more
The pharmacological management of asthma has changed considerably in recent decades, as it has come to be understood that it is a complex, heterogeneous disease with different phenotypes and endotypes. It is now clear that the goal of asthma treatment should be to achieve and maintain control of the
...
disease, as well as to minimize the risks (of exacerbations, disease instability, accelerated loss of lung function, and adverse treatment effects). That requires an approach that is personalized in terms of the pharmacological treatment, patient education, written action plan, training in correct inhaler use, and review of the inhaler technique at each office visit. A panel of 22 pulmonologists was invited to perform a critical review of recent evidence of pharmacological treatment of asthma and to prepare this set of recommendations, a treatment guide tailored to use in Brazil. The topics or questions related to the most significant changes in concepts, and consequently in the management of asthma in clinical practice, were chosen by a panel of experts. To formulate these recommendations, we asked each expert to perform a critical review of a topic or to respond to a question, on the basis of evidence in the literature. In a second phase, three experts discussed and structured all texts submitted by the others. That was followed by a third phase, in which all of the experts reviewed and discussed each recommendation. These recommendations, which are intended for physicians involved in the treatment of asthma, apply to asthma patients of all ages.
more
Time has seen management for Cystic Fibrosis (CF) advance drastically, most recently in the development of the disease-modifying triple combination therapy ivacaftor/tezacaftor/elexacaftor. There is currently limited evidence regarding both the global epidemiology of CF and access to this transforma
...
tive therapy - and therefore where needs are not being met. Therefore, this study aims to define gaps in access to CF treatment. The results show that a significant CF patient burden exists in countries where disease-modifying drugs are unavailable, and final figures are likely underestimates. This analysis shows the potential to improve rates of diagnosis and treatment for CF, so a higher percentage of patients receive the most effective triple combination treatment.
more

Procurement and supply management activities are fundamental to consistent and reliable access to essential medicines and health products. To reduce the impact of CVD, action needs to be taken to improve prevention, diagnosis, care and management of CVD diseases. Affordable essential medicines and t
...
echnologies to manage CVD disease must be available where and when they are required. Medicines and technologies need to be managed appropriately to ensure that the correct medicines are selected, procured in the right quantities, distributed to facilities in a timely manner, and handled and stored in a way that maintains their quality. This needs to be backed up by policies that enable sufficient quantities to be procured in order to reduce cost inefficiencies, ensure the reliability and security of the distribution system, and encourage the appropriate use of these health products. In order to avoid stock-outs and the disruption of treatment, all related activities need to be conducted in a timely manner, with performance continually monitored, and prompt action taken in response to problems that may arise. Additionally, medication must be dispensed correctly and used rationally by the healthcare provider and patient alike. The purpose of this guide is to explain the necessary steps.
more
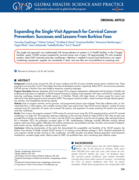
Background: Cervical cancer accounts for 23% of cancer incidence and 22% of cancer mortality among women in Burkina Faso. These proportions are more than 2 and 5 times higher than those of developed countries, respectively. Before 2010, cervical cancer prevention (CECAP) services in Burkina Faso wer
...
e limited to temporary screening campaigns.
Program Description: Between September 2010 and August 2014, program implementers collaborated with the Ministry of Health and professional associations to implement a CECAP program focused on coupling visual inspection with acetic acid (VIA) for screening with same-day cryotherapy treatment for eligible women in 14 facilities. Women with larger lesions or lesions suspect for cancer were referred for loop electrosurgical excision procedure (LEEP). The program trained providers, raised awareness through demand generation activities, and strengthened monitoring capacity.
Methods: Data on program activities, service provision, and programmatic lessons were analyzed. Three data collection tools, an individual client form, a client registry, and a monthly summary sheet, were used to track 3 key CECAP service indicators: number of women screened using VIA, proportion of women who screened VIA positive, and proportion of women screening VIA positive who received same-day cryotherapy.
Results: Over 4 years, the program screened 13,999 women for cervical cancer using VIA; 8.9% screened positive; and 65.9% received cryotherapy in a single visit. The proportion receiving cryotherapy on the same day started at a high of 82% to 93% when services were provided free of charge, but dropped to 51% when a user fee of $10 was applied to cover the cost of supplies. After reducing the fee to $4 in November 2012, the proportion increased again to 78%. Implementation challenges included difficulties tracking referred patients, stock-outs of key supplies, difficulties with machine maintenance, and prohibitive user fees. Providers were trained to independently monitor services, identify gaps, and take corrective actions.
Conclusions: Following dissemination of the results that demonstrated the acceptability and feasibility of the CECAP program, the Burkina Faso Ministry of Health included CECAP services in its minimum service delivery package in 2016. Essential components for such programs include provider training on VIA, cryotherapy, and LEEP; provider and patient demand generation; local equipment maintenance; consistent supply stocks; referral system for LEEP; non-prohibitive fees; and a monitoring data collection system.
more
There is a broad consensus nowadays that the Earth is warming up as a result of greenhouse gas emissions caused by anthropogenic activities. It is also clear that current trends in the fields of energy, development and population growth will lead to continuous and ever more dramatic climate change.
...
This is bound to affect the fundamental prerequisites for maintaining good health: clean air and water, sufficient food and adequate housing. The planet will warm up gradually, but the consequences of the extreme weather conditions such as frequent
storms, floods, droughts and heat-waves will have sudden onset and acute repercussions. It is widely accepted that climate change will have an impact on the spread of infectious diseases in Europe, which is likely to bring about new public health risks in the majority of cases. Transmission of infectious diseases depends on a number of factors, including climate and environmental elements. Foodborne and waterborne diseases, for instance, are associated with high temperatures. Disease-transmitting vectors (e.g. mosquitoes, sandflies and ticks) are highly sensitive to climate conditions, including temperature and humidity; their geographical distribution will widen as climate conditions change, potentially allowing them to spread into regions where they are not currently able to live.
The primary purpose of this manual on climate change and infectious diseases is to raise the awareness and the level of knowledge of health workers at national, regional and local levels in the former Yugoslav Republic of Macedonia on the health risks associated with climate change and infectious diseases. This manual was devel-
oped as part of the WHO Regional Office for Europe project, Protecting health from climate change: a seven–country initiative, implemented with financial support from the German Federal Ministry for the Environment, Nature Conservation and Nuclear Safety.
more
Infectious disease outbreaks and epidemics are increasing in frequency, scale and impact. Health care facilities can amplify the transmission of emerging infectious diseases or multidrug-resistant organisms (MDRO) within their settings and communities. Therefore, evidence-based infection prevention
...
and control (IPC) measures in health care facilities are critical for preventing and containing outbreaks, while still delivering safe, effective and quality health care. This toolkit is intended to support IPC improvements for outbreak management in all such facilities, both public and private throughout the health system. Specifically, this document systematically describes a framework of overarching principles to approach the preparedness, readiness and response outbreak management phases. The document also provides a toolkit of resource links to guide specific actions for each infectious disease and/or MDRO outbreak management phase at any health facility. This document is specifically tailored to an audience of stakeholders who establish and monitor health care facility-level IPC programs including: IPC focal points, epidemiologists, public health experts, outbreak response incident managers, facility-level IPC committee(s), safety and quality leads and managers, and other facility level IPC stakeholders.
more

KEY MESSAGES
Always talk to a GBV specialist first to understand what GBV services are available in your area. Some services may take the form of hotlines, a mobile app or other remote support.
Be aware of any other available services in your area. Identify services provided by humanitarian pa
...
rtners such as health, psychosocial support, shelter and non-food items. Consider services provided by communities such as mosques/ churches, women’s groups and Disability Service Organizations.
Remember your role. Provide a listening ear, free of judgment. Provide accurate, up-to-date information on available services. Let the survivor make their own choices. Know what you can and cannot manage. Even without a GBV actor in your area, there may be other partners, such as a child protection or mental health specialist, who can support survivors that require additional attention and support. Ask the survivor for permission before connecting them to anyone else. Do not force the survivor if s/he says no.
Do not proactively identify or seek out GBV survivors. Be available in case someone asks for support.
Remember your mandate. All humanitarian practitioners are mandated to provide non-judgmental and non-discriminatory support to people in need regardless of: gender, sexual orientation, gender identity, marital status, disability status, age, ethnicity/tribe/race/religion, who perpetrated/committed violence, and the situation in which violence was committed. Use a survivor-centered approach by practicing:
Respect: all actions you take are guided by respect for the survivor’s choices, wishes, rights and dignity.
Safety: the safety of the survivor is the number one priority.
Confidentiality: people have the right to choose to whom they will or will not tell their story. Maintaining confidentiality means not sharing any information to anyone.
Non-discrimination: providing equal and fair treatment to anyone in need of support.
If health services exist, always provide information on what is available. Share what you know, and most importantly explain what you do not. Let the survivor decide if s/he wants to access them. Receiving quality medical care within 72 hours can prevent transmission of sexually transmitted infections (STIs), and within 120 hours can prevent unwanted pregnancy.
Provide the opportunity for people with disabilities to communicate to you without the presence of their caregiver, if wished and does not endanger or create tension in that relationship.
If a man or boy is raped it does not mean he is gay or bisexual. Gender-based violence is based on power, not someone’s sexuality.
Sexual and gender minorities are often at increased risk of harm and violence due to their sexual orientation and/or gender identity. Actively listen and seek to support all survivors.
Anyone can commit an act of gender-based violence including a spouse, intimate partner, family member, caregiver, in-law, stranger, parent or someone who is exchanging money or goods for a sexual act.
Anyone can be a survivor of gender-based violence – this includes, but isn’t limited to, people who are married, elderly individuals or people who engage in sex work.
Protect the identity and safety of a survivor. Do not write down, take pictures or verbally share any personal/identifying information about a survivor or their experience, including with your supervisor. Put phones and computers away to avoid concern that a survivor’s voice is being recorded.
Personal/identifying information includes the survivor’s name, perpetrator(s) name, date of birth, registration number, home address, work address, location where their children go to school, the exact time and place the incident took place etc.
Share general, non-identifying information
To your team or sector partners in an effort to make your program safer.
To your support network when seeking self-care and encouragement.
more
Background: Cardiovascular disease (CVD), mainly heart attack and stroke, is the
leading cause of premature mortality in low and middle income countries (LMICs).
Identifying and managing individuals at high risk of CVD is an important strategy to prevent and control CVD, in addition to multisector
...
al population-based interventions to reduce CVD risk factors in the entire population.
Methods: We describe key public health considerations in identifying and managing individuals at high risk of CVD in LMICs.
Results: A main objective of any strategy to identify individuals at high CVD risk is to maximize the number of CVD events averted while minimizing the numbers of
individuals needing treatment. Scores estimating the total risk of CVD (e.g. ten-year risk of fatal and non-fatal CVD) are available for LMICs, and are based on the main CVD risk factors (history of CVD, age, sex, tobacco use, blood pressure, blood cholesterol and diabetes status). Opportunistic screening of CVD risk factors enables identification of persons with high CVD risk, but this strategy can be widely applied in low resource settings only if cost effective interventions are used (e.g. the WHO Package of Essential NCD interventions for primary health care in low resource settings package) and if treatment (generally for years) can be sustained, including continued availability ofaffordable medications and funding mechanisms that allow people to purchase medications without impoverishing them (e.g. universal access to health care). Thisalso emphasises the need to re-orient health systems in LMICs towards chronic diseases management.
Conclusion: The large burden of CVD in LMICs and the fact that persons with high
CVD can be identified and managed along cost-effective interventions mean that
health systems need to be structured in a way that encourages patient registration, opportunistic screening of CVD risk factors, efficient procedures for the management of chronic conditions (e.g. task sharing) and provision of affordable treatment for those with high CVD risk. The focus needs to be in primary care because that is where most of the population can access health care and because CVD programmes can be run effectively at this level.
more
The World Heart Federation (WHF) Roadmap series covers a large range of cardiovascular conditions. These Roadmaps identify potential roadblocks and their solutions to improve the prevention, detection and management of cardiovascular diseases and provide a generic global framework available for loca
...
l adaptation. A first Roadmap on raised blood pressure was published in 2015. Since then, advances in hypertension have included the publication of new clinical guidelines (AHA/ACC; ESC; ESH/ISH); the launch of the WHO Global HEARTS Initiative in 2016 and the associated Resolve to Save Lives (RTSL) initiative in 2017; the inclusion of single-pill combinations on the WHO Essential
Medicines’ list as well as various advances in technology, in particular telemedicine and mobile health. Given the substantial benefit accrued from effective interventions in the management of hypertension and their potential for scalability in low and middle-income countries (LMICs), the WHF has now revisited and updated the ‘Roadmap for raised BP’ as ‘Roadmap for hypertension’
by incorporating new developments in science and policy. Even though cost-effective lifestyle and medical interventions to prevent and manage hypertension exist, uptake is still low, particularly in resource-poor areas. This Roadmap examined the roadblocks pertaining to both the demand side (demographic and socio-economic factors, knowledge and beliefs, social relations, norms, and
traditions) and the supply side (health systems resources and processes) along the patient pathway to propose a range of possible solutions to overcoming them. Those include the development of population-wide prevention and control programmes; the implementation of opportunistic screening and of out-of-office blood pressure measurements; the strengthening of primary care and a greater focus on task sharing and team-based care; the delivery of people-centred care and stronger patient and carer education; and the facilitation of adherence to treatment. All of the above are dependent upon the availability and effective distribution of good quality, evidencebased, inexpensive BP-lowering agents.
more

Cholera is a transmissible diarrhoeal infection caused by Vibrio cholerae. Endemic and/or epidemic in over 40 countries (mainly in Africa and Asia), cholera continues to be a major global public health issue.
The World Health Organization (WHO) estimates that the number of cases reported worldwid
...
e represents in reality only 5 to 10% of actual cases.
This guide is intended for medical and non-medical staff responding to a cholera outbreak. It attempts to provide concrete answers to the questions and problems faced by staff, based on the recommendations of reference organisations, such as WHO and UNICEF, as well as Médecins Sans Frontières’ experience in the field.
It is divided into 8 chapters. Chapter 1, Cholera overview, outlines the epidemiological and clinical features of cholera. Chapter 2, Outbreak investigation, explains the method and stages of a field investigation, from the alert to implementation of initial activities. Chapter 3, Cholera control measures, details measures and tools to prevent and/or control cholera transmission and mortality in populations affected, or at risk of being affected, by an epidemic (curative care, prevention means and health promotion activities). Chapter 4, Strategies for epidemic response, addresses the roll-out strategies of the measures described in Chapter 3 which depend on context (e.g. urban, rural, endemic, non-endemic setting, etc.), resources and particular constraints. Chapter 5, Cholera case management, details the different stages of cholera treatment, from diagnosis through to cure.
Chapter 6, Setting up cholera treatment facilities, focuses on the installation of treatment facilities that vary in size and complexity according to operational requirements (treatment centres and units and oral rehydration points). Chapter 7, Organisation of cholera treatment facilities, describes the organisation of these specialized facilities in terms of human resources, supply, water, hygiene and sanitation, etc. Chapter 8, Monitoring and evaluation, presents the key data to be collected and analysed during an epidemic to facilitate a tailored response and evaluate its quality and effectiveness.
The guide includes various practical tools in the appendices to facilitate activities (e.g. water quality tests, job descriptions, documents, etc.). Moreover, the toolbox also contains additional tools in editable formats (individual patient file, cholera case register, pictograms).
Despite all efforts, it is possible that certain errors may have been overlooked in this guide. Please inform the authors of any errors detected.
To ensure that this guide continues to evolve while remaining adapted to field realities, please send any comments or suggestions.
more
Protecting Patients, Supporting Practitioners in Tandem.
HRI Global is an independent health consultancy which specialises in Whole Health System Strengthening in the public and private sector by implementing the 12-Pillar Clinical Governance Programme (12-PCGP) in primary, secondary and tertiary h
...
ealth facilities/institutions; by working with the management and staff of the institutions and with local and national government. The programme protects patients and supports practitioners in tandem, enabling the facilities to become clinically governed to deliver quality and patient-centered care.
HRI Global is the founder and lead implementer of the 12-Pillar Clinical Governance Programme, which was designed and piloted in Cross River State, Nigeria, in 2004. HRI Global’s home-grown version of Clinical Governance is suitable for low and middle income countries (LMICs) in both government and privately-owned health facilities.
more

How to take medicines safely
German Agency for Quality in Medicine (ÄZQ)
(2011)
C1
Patient information on safe medical treatment. Available in: Arabic, English, French, Russian, Spanish, Turkish, German.
This is the English version. For other language versions visit: http://www.patienten-information.de/kurzinformationen/arzneimi
...
ttel-und-impfungen/sichere-arzneimitteltherapie
more
Medikamente sicher einnehmen (Arabic)
Ärztliches Zentrum für Qualität in der Medizin (ÄZQ)
(2011)
C1
Patienteninformation „Sichere Arzneimitteltherapie“ – Arabische Übersetzung. Broschüre auch erhältlich in: Deutsch, Englisch, Französisch, Russisch, Türkisch, Spanisch.
Patient information "Safe Medical Therapy " - Arabic translation. B
...
rochure also available in: German, English, French, Russian, Turkish, Spanish.
Für andere Sprachversionen, siehe auch / For other language versions go to: http://www.patienten-information.de/kurzinformationen/arzneimittel-und-impfungen/sichere-arzneimitteltherapie
more