Filter
2698
Filtered Results: 2698
Text search:
Maledives
Featured
Recommendations
211
New Publications
484
Language
Document type
No document type
1086
Studies & Reports
567
Guidelines
396
Fact sheets
164
Strategic & Response Plan
139
Manuals
102
Training Material
59
Infographics
55
Resource Platforms
32
Online Courses
25
Brochures
22
Videos
21
Situation Updates
18
Dashboards/Maps
11
App
1
Countries / Regions
Global
454
Congo, Democratic Republic of
143
Senegal
134
Africa
112
Burkina Faso
93
Benin
87
Haiti
56
Guinea
48
Cameroon
45
South–East Asia Region
42
West and Central Africa
41
Asia
39
Latin America and the Carribbean
39
Central African Republic
36
Mali
33
Madagascar
32
Côte d’Ivoire / Ivory Coast
28
India
28
Rwanda
22
East and Southern Africa
22
Niger
20
Nepal
19
Middle East and North Africa
19
North America
18
Togo
17
South Africa
16
Chad
16
Western and Central Europe
11
Bangladesh
11
Ukraine
9
France
9
Ethiopia
7
Indonesia
7
Syria
6
Burundi
6
Malawi
6
Eastern Europe
6
Brazil
6
Russia
6
Liberia
6
Sierra Leone
5
Congo-Brazzaville
5
Mozambique
5
Germany
5
Western Pacific Region
5
Eastern Europe and Central Asia
5
Sri Lanka
5
Yemen
5
Nigeria
4
Canada
4
Afghanistan
4
Morocco
4
USA
4
Djibouti
4
Angola
4
Somalia
4
Pakistan
4
Kenya
3
Ghana
3
China
3
Zimbabwe
3
Cambodia
3
Guinea-Bissau
3
Tanzania
3
Luxembourg
3
Belgium
3
Bolivia
3
Uganda
3
Namibia
3
South Sudan
3
Switzerland
2
Thailand
2
Mauritania
2
Saudi Arabia
2
Maldives
2
Egypt
2
Sudan
2
Bhutan
2
Zambia
2
Iraq
2
Ecuador
2
Myanmar / Burma
2
North Korea
1
Timor Leste/ East Timor
1
Mexico
1
Turkey
1
Gambia
1
Singapore
1
Austria
1
Philippines
1
Gabon
1
Jamaica
1
Tunisia
1
United Kingdom
1
Algeria
1
Southern Africa
1
Barbados
1
United Arab Emirates
1
Argentina
1
Vietnam
1
Georgia
1
Poland
1
Botswana
1
Bahamas
1
Guatemala
1
Authors & Publishers
Publication Years
Category
Public Health
815
Countries
707
Clinical Guidelines
432
Women & Child Health
125
Key Resources
97
Capacity Building
55
Pharmacy & Technologies
30
Toolboxes
NCDs
568
COVID-19
224
Rapid Response
144
Mental Health
131
Ebola
97
HIV
82
TB
73
NTDs
72
Caregiver
69
Disability
55
Planetary Health
51
Cholera
46
AMR
38
Zika
32
Refugee
29
Pharmacy
27
Natural Hazards
24
Global Health Education
24
Polio
20
Conflict
13
Health Financing Toolbox
11
Social Ethics
7
Typhoon
3
Specific Hazards
1
Health Financing
1
Hypertension, also known as high or raised blood pressure, is a condition in which the blood vessels have persistently raised pressure. Blood is carried from the heart to all parts of the body in the vessels. Each time the heart beats, it pumps blood into the vessels. Blood pressure is created by th...
Background
Cardiovascular diseases (CVDs) are one of the global leading causes of concern due to the rising prevalence and consequence of mortality and disability with a heavy economic burden. The objective of the current study was to analyze the trend in CVD incidence, mortality, and mortality-to-...

The South African (SA) guidelines for cardiac patients for non-cardiac surgery were developed to address the need for cardiac risk assessment and risk stratification for elective non-cardiac surgical patients in SA, and more broadly in Africa.
The guidelines were developed by updating the Canadian ...
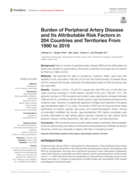
Background: Data on burden of peripheral artery disease (PAD) and its attributable risk factors are valuable for policymaking. We aimed to estimate the burden and risk factors for PAD from 1990 to 2019.
Methods: We extracted the data on prevalence, incidence, death, years lived with disability (YLD...
This guideline provides updated, evidence-informed guidance on the percentage of total fat in the diet to reduce the risk of unhealthy weight gain.
This guideline is intended for a wide audience involved in the development, design and implementation of policies and programmes in nutrition and pub...

Vaccines are powerful weapons in the fight against pandemic viruses as shown by responses to both the 2009 H1N1 influenza and the COVID-19 pandemics. However, planning for accessing, allocating and deploying vaccines in a pandemic situation is a complex endeavour, beset with multiple challenges at a...
La forte augmentation des taux de surpoids et d’obésité1 constitue une menace pour la santé de milliards
de personnes dans le monde. En 2016, plus de 1,9 milliard d’adultes âgés de 18 ans ou plus étaient en surpoid
Las tasas cada vez mayores de sobrepeso y obesidad son una amenaza para la salud de miles de millones
de personas en todo el mundo. En 2016, más de 1900 millones de mayores de 18 años tenían sobrepeso , de los cuales más de 600 millones eran obesos. En 2020, más de 38 millones de menores de 5 ...

What you should do as head of school or child centre to prevent cholera:
Educate all staff and pupils on the common cholera transmission routes and how to prevent it.
Educate all kitchen staff on how to handle food and cooking utensils. Emphasis the key points below:
o All kitchen staff MUST wa...
UNICEF: Protecting Ourselves from Cholera
recommended
This flipchart is a visual support for community workers, health workers, emergency workers, and in general all staff conducting face-to-face communication in response to a cholera outbreak.
How to use it?
The flipchart is intended as a support for animating individual or group discussions on ...
Cholera is an acute gastrointestinal infection caused by the bacterium Vibrio Cholerae serogroup O1 or O139, and is often linked to unsafe drinking water, lack of proper sanitation and personal hygiene. It adversely affects mostly the poor and vulnerable populations in countries, which are already d...

Cholera is a transmissible diarrhoeal infection caused by Vibrio cholerae. Endemic and/or epidemic in over 40 countries (mainly in Africa and Asia), cholera continues to be a major global public health issue.
The World Health Organization (WHO) estimates that the number of cases reported worldwid...

Global cardiovascular disease (CVD) burden is high and rising, especially in low-income and middle-income countries (LMICs). Focussing on 45 LMICs, we aimed to determine (1) the adult population’s median 10-year predicted CVD risk, including its variation within countries by socio-demographic char...
Myocardial infarctions are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI), based on changes in ECG. When blood flow to a part of the heart stops or the heart is injured and fails to receive enough oxygen required for its adequate functioning the conditi...

WHO has published the first-ever guidance on the clinical management of diphtheria. The only previously available guidance was an operational protocol. The new guidance followed the rigorous process for developing guidance at WHO.
It addresses the use of Diphtheria Antitoxin (DAT) in the treatmen...

Delivery of comprehensive arrhythmia care requires the simultaneous presence of many resources. These include complex hospital infrastructure, expensive implantable equipment, and expert personnel. In many low- and middle-income countries (LMICs), at least 1 of these components is often missing, res...
Heart failure is an important global health problem, and the associated public health and economic effect is increasing across all societies and geographies.
Epidemiological studies have estimated that there are more than 25 million patients with heart failure globally, and population-based studie...

Background
Noncommunicable diseases are major contributors to morbidity and mortality worldwide. Modifying the risk factors for these conditions, such as physical inactivity, is thus essential. Addressing the context or circumstances in which physical activity occurs may promote physical activity a...
Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among...