Filter
200
Featured
1
6
Language
Document type
84
30
21
19
12
8
7
6
5
3
1
1
1
1
Countries
17
14
11
8
2
2
2
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Authors & Publishers
Publication Years
Category
81
41
39
18
1

Cardiovascular disease (CVD) describes a group of conditions that affect your heart or blood vessels. Cardiovascular events like heart attacks and strokes are very serious.

The Children’s Cardiac Foundation deals with a wide rage of stakeholders from parents of children affected by CHD, to corporates and grant makers. Before contacting us, please read the relevant sections below as your questions may have already been answered.
Cardiovascular disease (CVD) is the leading cause of death in the Americas and raised blood pressure accounts for over 50% of CVD. In the Americas over a quarter of adult women and four in ten adult men have hypertension and the diagnosis, treatment and control are suboptimal. In 2021, the World Hea
...

This study was aimed to ascertain the clinical profile and management of patients with ischemic heart disease (IHD) and/or peripheral artery disease (PAD). In this observational and cross-sectional study developed in 80 hospitals throughout Spain, consecutive adults with stable IHD and/or PAD were i
...

Webpage about Atherosclerosis, addressing symptoms, diagnosis, causes and risk factors, prevention, treatment, living with the disease.

Webpage about Atherosclerosis, addressing symptoms, diagnosis, causes and risk factors, prevention, treatment, living with the disease.

Atherosclerosis is the build-up of fatty material (atheroma) inside your arteries. It's a potentially serious condition that causes most heart attacks and strokes but often goes unnoticed.

Cardiovascular disease (CVD) is a general term for conditions affecting the heart or blood vessels.
It's usually associated with a build-up of fatty deposits inside the arteries (atherosclerosis) and an increased risk of blood clots.
It can also be associated with damage to arteries in organs such
...

Peripheral arterial disease (PAD) in the legs or lower extremities is the narrowing or blockage of the vessels that carry blood from the heart to the legs. It is primarily caused by the buildup of fatty plaque in the arteries, which is called atherosclerosis. PAD can happen in any blood vessel, but
...

Treatment plan
This guide for patients aims to provide you with an overview of the latest evidence-based recommendations for the prevention of cardiovascular disease. In particular, it should help you to understand:
• how cardiovascular disease risk is assessed
• the importance of lifestyle modifications for
...
The first step toward heart health is understanding your risk of heart disease. Your risk depends on many factors, some of which are changeable and others that are not. Risk factors are conditions or habits that make a person more likely to develop a disease. These risk factors may be different for
...
Background
In the prevention of cardiovascular disease, a WHO target is that at least 50% of eligible people use statins. Robust evidence is needed to monitor progress towards this target in low-income and middle-income countries (LMICs), where most cardiovascular disease deaths occur. The objectiv
...
Background: Atherosclerotic cardiovascular diseases (ASCVD) including myocardial infarction, stroke and peripheral arterial disease continue to be major causes of premature death, disability and healthcare expenditure globally. Preventing the accumulation of cholesterol-containing atherogenic lipopr
...
ABSTRACT
More than 500 million people worldwide live with cardiovascular disease (CVD). Health systems today face fundamental challenges in delivering optimal care due to ageing populations, healthcare workforce constraints, financing, availability and affordability of CVD medicine, and service del
...
In 2015, the United Nations set important targets to reduce premature
cardiovascular disease (CVD) deaths by 33% by 2030. Africa disproportionately
bears the brunt of CVD burden and has one of the highest risks of dying
from non-communicable diseases (NCDs) worldwide. There is currently
an epide
...
Heart failure (HF) is a leading global public health problem with >64 million prevalent cases globally. Patients with HF with reduced ejection fraction (HFrEF) from low- and middle-income countries experience a 22% to 58% higher 1-year mortality rate than those in high-income countries.1 Guideline-d
...
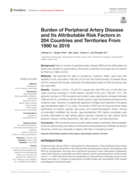
Background: Data on burden of peripheral artery disease (PAD) and its attributable risk factors are valuable for policymaking. We aimed to estimate the burden and risk factors for PAD from 1990 to 2019.
Methods: We extracted the data on prevalence, incidence, death, years lived with disability (YLD
...
Myocardial infarctions are generally clinically classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI), based on changes in ECG. When blood flow to a part of the heart stops or the heart is injured and fails to receive enough oxygen required for its adequate functioning the conditi
...

Delivery of comprehensive arrhythmia care requires the simultaneous presence of many resources. These include complex hospital infrastructure, expensive implantable equipment, and expert personnel. In many low- and middle-income countries (LMICs), at least 1 of these components is often missing, res
...