Filter
9800
Filtered Results: 9800
Text search:
et
al,
Featured
Recommendations
748
New Publications
1979
Language
Document type
No document type
4891
Studies & Reports
2113
Guidelines
1385
Manuals
450
Fact sheets
271
Strategic & Response Plan
260
Training Material
180
Infographics
81
Situation Updates
51
Resource Platforms
48
Brochures
33
Online Courses
17
Videos
10
Dashboards/Maps
7
App
3
Countries / Regions
Global
431
Latin America and the Carribbean
286
India
220
Western and Central Europe
198
Kenya
189
South Africa
183
Russia
182
Germany
175
Africa
153
Ethiopia
147
Brazil
133
Paraguay
126
Ukraine
120
Malawi
118
Nigeria
117
Senegal
117
Nepal
116
Venezuela
115
Sierra Leone
112
Congo, Democratic Republic of
106
Uganda
104
Zambia
100
Eastern Europe
99
Syria
94
Liberia
92
Bangladesh
92
Tanzania
89
Colombia
87
Myanmar / Burma
85
Argentina
82
Burkina Faso
75
Haiti
74
Mozambique
73
Ghana
72
Rwanda
70
Indonesia
66
Middle East and North Africa
63
Guinea
59
Peru
58
West and Central Africa
57
Benin
56
Eastern Europe and Central Asia
56
Asia
50
South–East Asia Region
48
Zimbabwe
47
Philippines
47
Chile
44
East and Southern Africa
43
Cameroon
42
Yemen
42
Ecuador
39
Namibia
35
Bolivia
33
Lesotho
32
South Sudan
30
Angola
30
Mali
28
Cambodia
28
Madagascar
25
Central African Republic
24
Spain
24
El Salvador
23
Botswana
21
Côte d’Ivoire / Ivory Coast
20
Pakistan
20
Somalia
19
Sudan
19
Guinea-Bissau
18
Niger
18
China
18
USA
16
Jordan
16
Lebanon
16
Western Pacific Region
16
Tajikistan
16
Afghanistan
15
Chad
15
Mexico
15
Thailand
14
Sri Lanka
13
Vietnam
13
Iraq
12
Eswatini/ Swaziland
11
Albania
11
Southern Africa
11
Portugal
11
Italy
10
North America
10
Egypt
9
Guatemala
9
Kyrgyzstan
9
Kazakhstan
9
Palestine
8
France
8
Saudi Arabia
7
Togo
7
Burundi
7
Honduras
7
Libya
7
Canada
7
Georgia
7
Turkey
6
Dominican Republic
6
Switzerland
6
Laos
6
Congo-Brazzaville
6
United Kingdom
6
Belarus
6
Morocco
5
Papua New Guinea
5
North Macedonia
5
Nicaragua
5
Armenia
5
Estonia
5
Moldova
5
Iran
5
Uruguay
5
Tunisia
5
Greece
4
Djibouti
4
Timor Leste/ East Timor
4
Malaysia
3
Singapore
3
Poland
3
Qatar
3
Romania
3
Gabon
3
Turkmenistan
3
Jamaica
3
Japan
3
Belgium
3
Israel
3
Mauritania
2
Austria
2
Hungary
2
Luxembourg
2
Fiji
2
Uzbekistan
2
Denmark
2
Algeria
2
Bosnia and Herzegovina
2
Ireland
1
Serbia
1
Croatia
1
Cuba
1
Other region
1
Solomon Islands
1
Bhutan
1
North Korea
1
Mongolia
1
Bulgaria
1
Lithuania
1
Slovakia
1
Mauritius
1
Morocco
1
French Guyana
1
Latvia
1
Authors & Publishers
Publication Years
Category
Countries
3382
Clinical Guidelines
753
Public Health
527
Women & Child Health
488
Key Resources
360
Capacity Building
167
Pharmacy & Technologies
86
Toolboxes
COVID-19
1177
Mental Health
982
HIV
738
TB
650
Planetary Health
457
Disability
306
NTDs
301
NCDs
285
Caregiver
281
Refugee
252
AMR
248
Ebola
218
Rapid Response
207
Conflict
181
Global Health Education
151
Health Financing Toolbox
135
Pharmacy
123
Zika
86
Natural Hazards
84
Cholera
49
Social Ethics
43
Polio
42
Specific Hazards
42
Typhoon
2
Health Financing
2
South Sudan
1
Background: Disbursements of development assistance for health (DAH) have risen substantially during the past several decades. More recently, the international community's attention has turned to other international challenges, introducing uncertainty about the future of disbursements for DAH.
Meth...
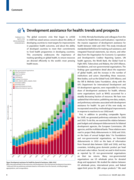
The global economic crisis that began to unfold in 2008 has raised serious concerns about the ability of developing countries to meet targets for improvements in population health outcomes, and about the ability of developed countries to meet their commitments to fund health programmes in developing...
Background: Investing in the health workforce is key to achieving the health-related Sustainable Development Goals. However, achieving these Goals requires addressing a projected global shortage of 18 million health workers (mostly in low- and middle-income countries). Within that context, in 2016, ...

Background: A recent report by the Institute for Health Metrics and Evaluation (IHME) highlights that mental health receives little attention despite being a major cause of disease burden. This paper extends previous assessments of development assistance for mental health (DAMH) in two significant w...
The International Conference on Population and Development in 1994 set targets for donor funding to support family planning programmes, and recent initiatives such as FP2020 have renewed focus on the need for adequate funding to rights-based family planning. Disbursements supporting family planning ...

Background:Neonatal mortality accounts for 43% of global under-five deaths and is decreasing more slowly than maternal or child mortality. Donor funding has increased for maternal, newborn, and child health (MNCH), but no analysis to date has disaggregated aid for newborns. We evaluated if and how a...
Background: The need for sufficient and reliable funding to support health policy and systems research (HPSR) in low- and middle-income countries (LMICs) has been widely recognised. Currently, most resources to support such activities come from traditional development assistance for health (DAH) don...

Between 2012 and 2016, development assistance for HIV/AIDS decreased by 20·0%; domestic financing is therefore critical to sustaining the response to HIV/AIDS. To understand whether domestic resources could fill the financing gaps created by declines in development assistance, we aimed to track spe...

he global architecture for providing development assistance for health (DAH)
has become increasing complex in the last decade, with many new funding agencies entering the health sector.
This study presents a detailed picture of European Union (EU) and EU member state originating DAH
between 2006 ...
Four initiatives have estimated the value of aid for reproductive, maternal, newborn, and child health
(RMNCH): Countdown to 2015, the Institute for Health Metrics and Evaluation (IHME), the Muskoka Initiative, and
the Organisation for Economic Co-operation and Development (OECD) policy marker. We...
To provide information on trends on official development assistance (ODA) disbursement patterns for
reproductive health activities in 18 conflict-affected countries
Donor financing to low- and middle-income countries for reproductive, maternal, newborn, and child health increased substantially from 2008 to 2013. However, increased spending by donors might not improve outcomes, if funds are delivered in ways that undermine countries’ public financial managemen...

Reproductive health needs are particularly acute in countries affected by armed conflict. Reliable information
on aid investment for reproductive health in these countries is essential for improving the efficiency and effectiveness of
aid. The purpose of this study was to analyse official developm...

Official development assistance (ODA) is one of the most important means for donor countries to foster diplomatic relations with low- and middle-income countries and contribute to the welfare of the international community.Objective: This study estimated the sectoral allocation of

A country’s ability to manage a crisis depends on its level of resilience. Efforts are made to clarify the concept of health system resilience, but its operationalisation remains little studied. In the present research, we described the capacity of the local healthcare system in the Islamic Republ...

Background
Four methods have previously been used to track aid for reproductive, maternal, newborn, and child health (RMNCH). At a meeting of donors and stakeholders in May, 2018, a single, agreed method was requested to produce accurate, predictable, transparent, and up-to-date estimates that coul...
A general consensus exists that as a country develops economically, health spending per capita rises and the share of that spending that is prepaid through government or private mechanisms also rises. However, the speed and magnitude of these changes vary substantially across countries, even at simi...
Introduction
In 2017, development assistance for health (DAH) comprised 5.3% of total health spending in lowincome countries. Despite the key role DAH plays in global health-spending, little is known about the characteristics of assistance that may be associated with committed assistance that is a...
Unpreparedness of health professionals to address non-communicable diseases (NCD) at peripheral health facilities is a critical health system challenge in Mozambique. To address this weakness and decentralize NCD care, training of the primary care workforce is needed. We describe our experience in t...
Cardiovascular disease (CVD) is the leading cause of global deaths, with the majority occurring in low- and middle-income countries (LMIC). The primary and secondary prevention of CVD is suboptimal throughout the world, but the evidence-practice gaps are much more pronounced in LMIC. Barriers at the...